Dd Form 2870 Tricare
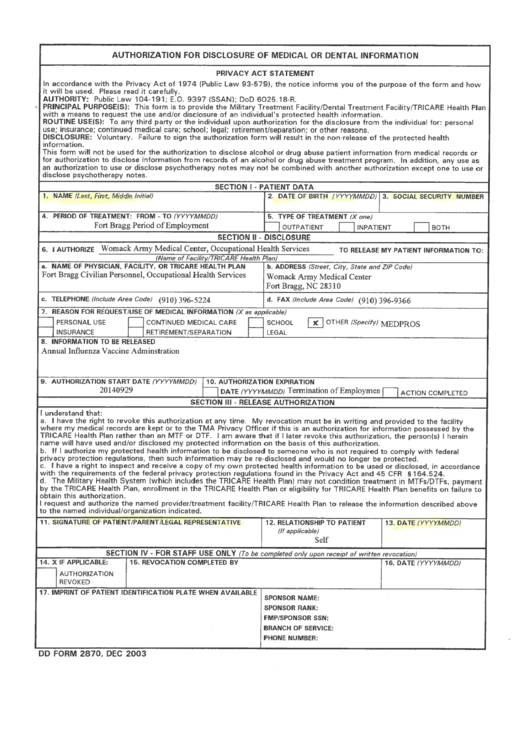
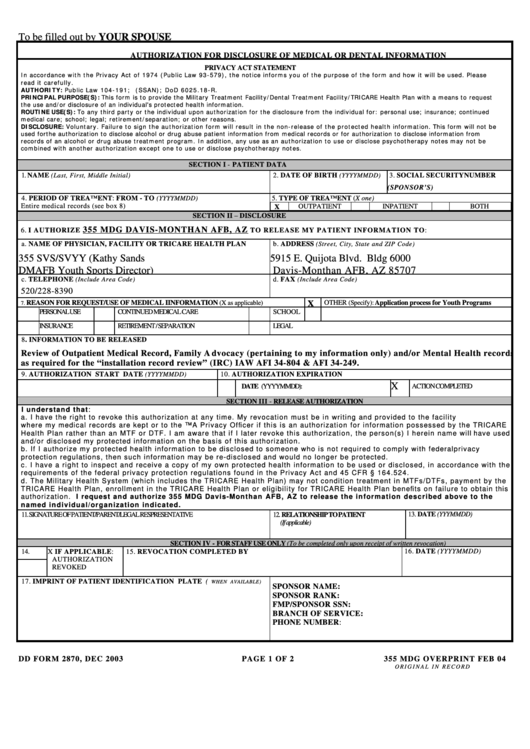
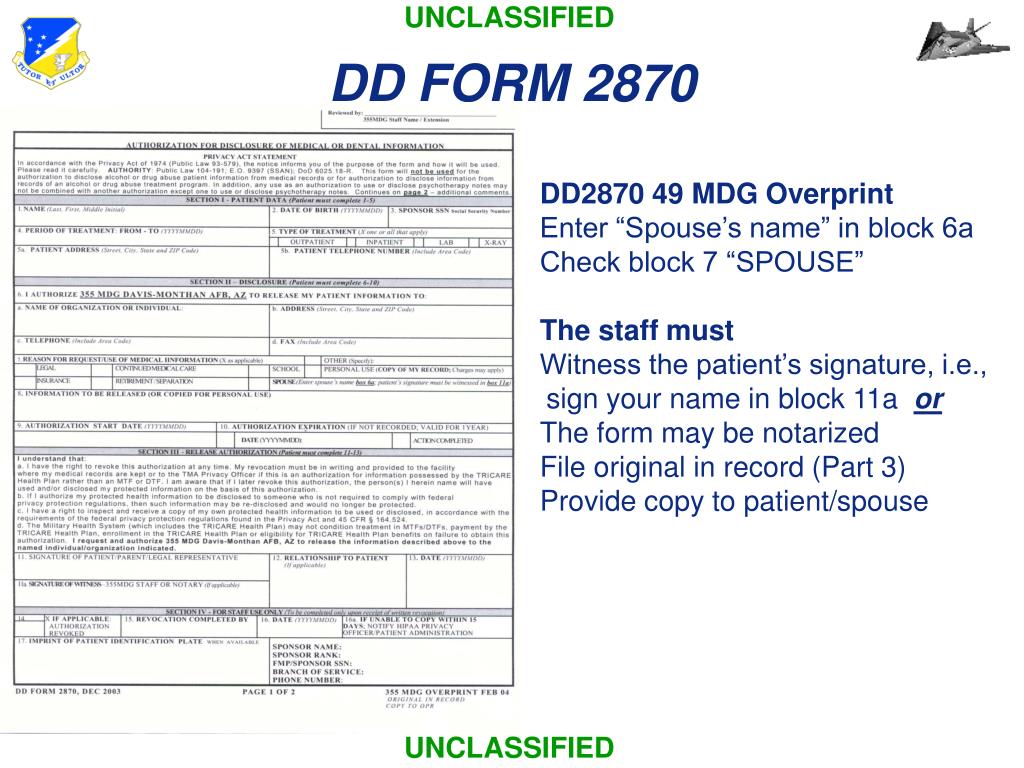
Dd Form 2870 Tricare - Web by the tricare health plan, enrollment in the tricare health plan or eligibility for tricare health plan benefits on failure to. Web submit the completed dd form 2870 to the relevant military hospitals or clinics. Patient’s name in this block. Web authorization for disclosure of medical or dental information dd form 2870, dec 2003 adobe professional 8.0 Indicate the dates of treatment you are looking for or if you want everything put “all time periods”. Iach form 2870 (2023) for the following to be included, initial. Web instructions for filling out dd form 2870 (authorization for disclosure of medical or dental information) patient name patient date of birth patient ssn Download standard form (sf) 180 and follow the. Patient’s date of birth block 3: Short requests (less than 10 pages) can be processed on the spot, to include such records as:
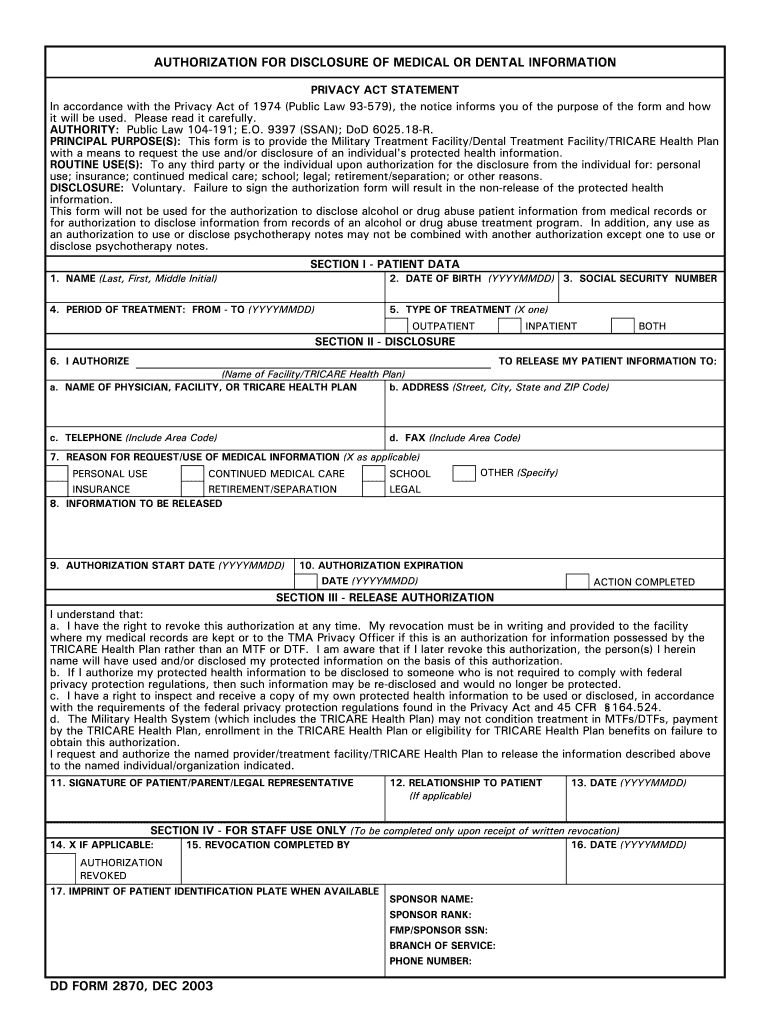
Patient’s complete social security number in this block. Iach form 2870 (2023) for the following to be included, initial. Lab results immunization records radiology reports physicals (school, sports, etc.) electronic progress/office visit note (s) Web authorization for disclosure of medical or dental information dd form 2870, dec 2003 adobe professional 8.0 Patient’s date of birth in this block. Patient’s name in this block. Short requests (less than 10 pages) can be processed on the spot, to include such records as: Web instructions for filling out dd form 2870 (authorization for disclosure of medical or dental information) patient name patient date of birth patient ssn Web to complete the dd form 2870, please follow the below instructions: Web submit the completed dd form 2870 to the relevant military hospitals or clinics.
Patient’s name in this block. Web to complete the dd form 2870, please follow the below instructions: Indicate the date(s) of treatment you (the patient) wants released block 5: Dd form 2870, authorization for disclosure of. Web by the tricare health plan, enrollment in the tricare health plan or eligibility for tricare health plan benefits on failure to. Web submit the completed dd form 2870 to the relevant military hospitals or clinics. Download standard form (sf) 180 and follow the. Web for your convenience, patients can pick up and complete, as well as drop off completed dd form 2870’s at the roi quick stop. Indicate the dates of treatment you are looking for or if you want everything put “all time periods”. Web authorization for disclosure of medical or dental information (dd form 2870) your provider or contractor will use this form is to get your permission to share your protected health information to a third party for personal use;

Dd form 2870 authorization for disclosure of medical or by
Web instructions for filling out dd form 2870 (authorization for disclosure of medical or dental information) patient name patient date of birth patient ssn Web authorization for disclosure of medical or dental information (dd form 2870) your provider or contractor will use this form is to get your permission to share your protected health information to a third party for.
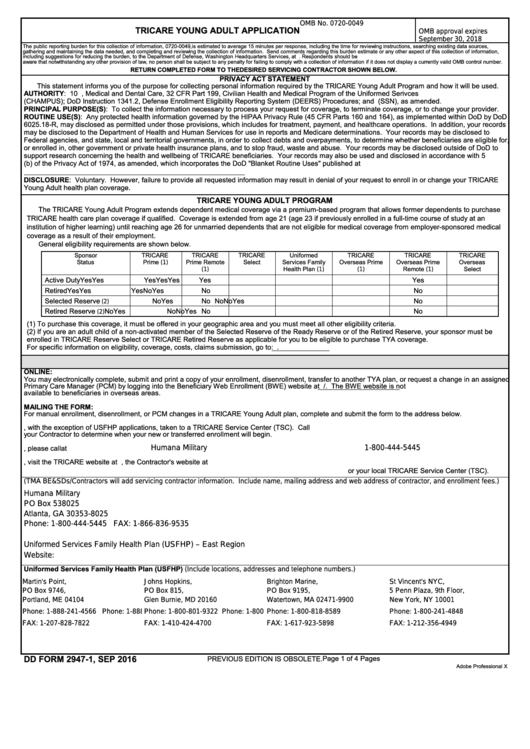
Fillable Dd Form 29471 Tricare Young Adult Application printable pdf
Patient’s name in this block. Dd form 2870, authorization for disclosure of. Web authorization for disclosure of medical or dental information dd form 2870, dec 2003 adobe professional 8.0 Indicate the dates of treatment you are looking for or if you want everything put “all time periods”. Web to complete the dd form 2870, please follow these instructions carefully:

DD Form 2854 Download Fillable PDF or Fill Online TRICARE Plus
Web authorization for disclosure of medical or dental information (dd form 2870) your provider or contractor will use this form is to get your permission to share your protected health information to a third party for personal use; Lab results immunization records radiology reports physicals (school, sports, etc.) electronic progress/office visit note (s) Indicate the date(s) of treatment you (the.
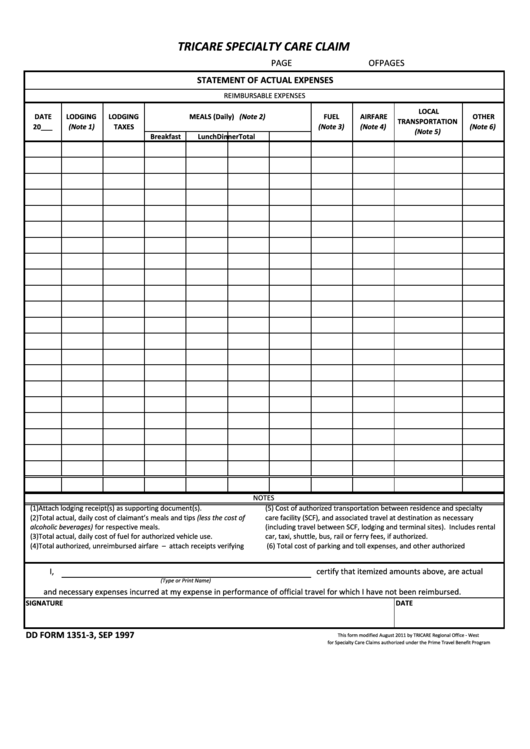
Fillable Dd Form 13513, Tricare Specialty Care Claim printable pdf
Web to complete the dd form 2870, please follow these instructions carefully: Short requests (less than 10 pages) can be processed on the spot, to include such records as: Patient’s name in this block. Indicate the dates of treatment you are looking for or if you want everything put “all time periods”. Iach form 2870 (2023) for the following to.
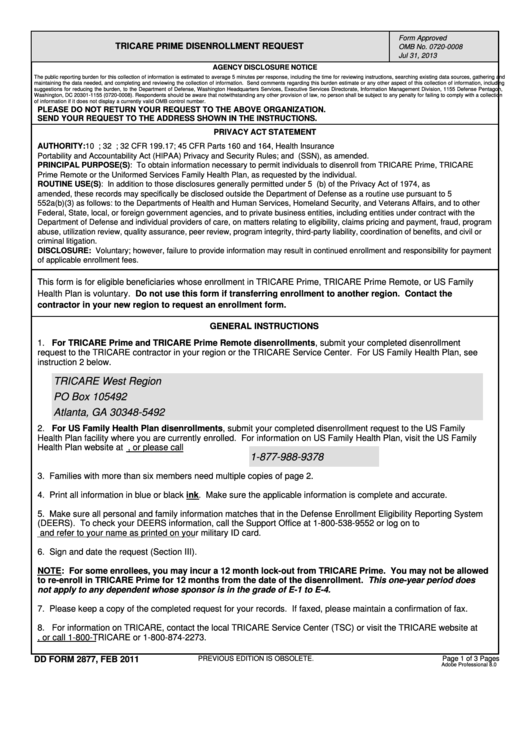
Fillable Dd Form 2877 Tricare Prime Disenrollment Request printable
Lab results immunization records radiology reports physicals (school, sports, etc.) electronic progress/office visit note (s) Web by the tricare health plan, enrollment in the tricare health plan or eligibility for tricare health plan benefits on failure to. Web to complete the dd form 2870, please follow these instructions carefully: Web authorization for disclosure of medical or dental information (dd form.
Dd Form 2870 Army Pubs Army Military
Web for your convenience, patients can pick up and complete, as well as drop off completed dd form 2870’s at the roi quick stop. Patient’s complete social security number in this block. Short requests (less than 10 pages) can be processed on the spot, to include such records as: Web to complete the dd form 2870, please follow these instructions.
Download Dd Form 2870 Authorization For Disclosure Of Medical Or
Download standard form (sf) 180 and follow the. Web by the tricare health plan, enrollment in the tricare health plan or eligibility for tricare health plan benefits on failure to. Web to complete the dd form 2870, please follow the below instructions: Web for your convenience, patients can pick up and complete, as well as drop off completed dd form.
Download Dd Form 2870 Authorization For Disclosure Of Medical Or
Download standard form (sf) 180 and follow the. Web authorization for disclosure of medical or dental information (dd form 2870) your provider or contractor will use this form is to get your permission to share your protected health information to a third party for personal use; Indicate the dates of treatment you are looking for or if you want everything.

Dd Form 2870 Printable Improve your tax management airSlate
Short requests (less than 10 pages) can be processed on the spot, to include such records as: Patient’s complete social security number in this block. Iach form 2870 (2023) for the following to be included, initial. Web for your convenience, patients can pick up and complete, as well as drop off completed dd form 2870’s at the roi quick stop..
PPT TRICARE BRIEFING PowerPoint Presentation, free download ID4453403
Download standard form (sf) 180 and follow the. Web authorization for disclosure of medical or dental information dd form 2870, dec 2003 adobe professional 8.0 Web by the tricare health plan, enrollment in the tricare health plan or eligibility for tricare health plan benefits on failure to. Web to complete the dd form 2870, please follow these instructions carefully: Patient’s.
Patient’s Complete Social Security Number In This Block.
Web authorization for disclosure of medical or dental information dd form 2870, dec 2003 adobe professional 8.0 Web by the tricare health plan, enrollment in the tricare health plan or eligibility for tricare health plan benefits on failure to. Patient’s date of birth block 3: Iach form 2870 (2023) for the following to be included, initial.
Patient’s Name In This Block.
Web instructions for filling out dd form 2870 (authorization for disclosure of medical or dental information) patient name patient date of birth patient ssn Dd form 2870, authorization for disclosure of. Web for your convenience, patients can pick up and complete, as well as drop off completed dd form 2870’s at the roi quick stop. Web authorization for disclosure of medical or dental information (dd form 2870) your provider or contractor will use this form is to get your permission to share your protected health information to a third party for personal use;
Indicate The Dates Of Treatment You Are Looking For Or If You Want Everything Put “All Time Periods”.
Web to complete the dd form 2870, please follow the below instructions: Short requests (less than 10 pages) can be processed on the spot, to include such records as: Web to complete the dd form 2870, please follow these instructions carefully: Lab results immunization records radiology reports physicals (school, sports, etc.) electronic progress/office visit note (s)
Download Standard Form (Sf) 180 And Follow The.
Indicate the date(s) of treatment you (the patient) wants released block 5: Web submit the completed dd form 2870 to the relevant military hospitals or clinics. Patient’s date of birth in this block.