Dcps Dental Form
Dcps Dental Form - Child’s clinical examination (to be completed by the dental provider)date of exam __________________________ (please use key to document all findings on line next to each tooth) All employees are eligible for dental and vision options outlined in the dental/optical section below. Please indicate the ward of your home address, list primary care provider, dental provider, and type of dental insurance. Web health physicals and oral health assessments are required annually. Please indicate the ward of your home address, list primary care provider, dental provider, and type of dental insurance. Take this form to the student's dental provider. • return fully completed and signed form to the student's school/child care facility. If the child has no dental provider and is uninsured, Students also must be current with their immunizations to attend school. Web district of columbia oral health (dental provider) assessment form part 1.
Child’s clinical examination (to be completed by the dental provider)date of exam __________________________ (please use key to document all findings on line next to each tooth) Web district of columbia oral health (dental provider) assessment form part 1. For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Web instructions • complete part 1 below. Web district of columbia oral health (dental provider) assessment form parent/guardian instructions: Take this form to the student's dental provider. Web universal health certificate use this form to report your child’s physical health to their school/child care facility. Students also must be current with their immunizations to attend school. Web district of columbia oral health (dental provider) assessment form. Amharic (አማርኛ) (link is external) chinese (中文) (link is external) english.
Schools must verify every student’s immunization compliance as part of enrollment and attendance (see the school immunization policy for more details). • return fully completed and signed form to the student's school/child care facility. Child’s personal information part 2. For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Part 1:please complete all sections including child’s race or ethnicity. Web district of columbia oral health (dental provider) assessment form part 1. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web instructions • complete part 1 below. Students also must be current with their immunizations to attend school. Amharic (አማርኛ) (link is external) chinese (中文) (link is external) english.
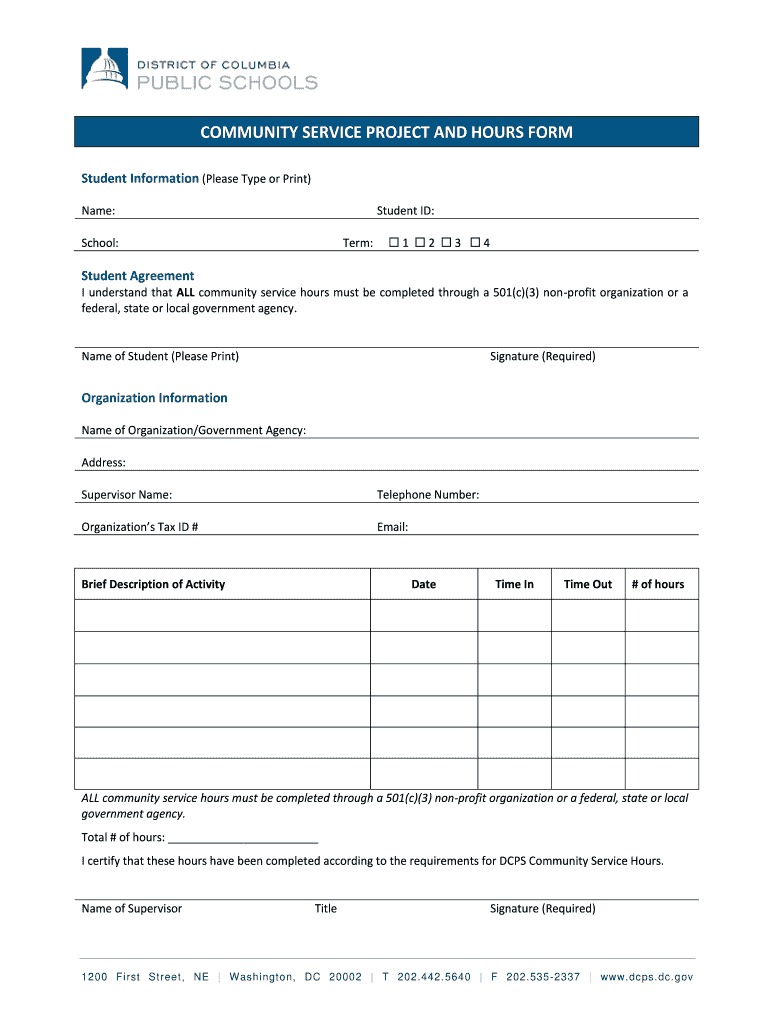
Dcps Community Service Form Fill Online, Printable, Fillable, Blank
Schools must verify every student’s immunization compliance as part of enrollment and attendance (see the school immunization policy for more details). Please indicate the ward of your home address, list primary care provider, dental provider, and type of dental insurance. Child’s clinical examination (to be completed by the dental provider)date of exam __________________________ (please use key to document all findings.
benefits.htm
Get everything done in minutes. For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Web district of columbia oral health (dental provider) assessment form. Students also must be current with their immunizations to attend school. Student information (to be completed by parent/guardian)
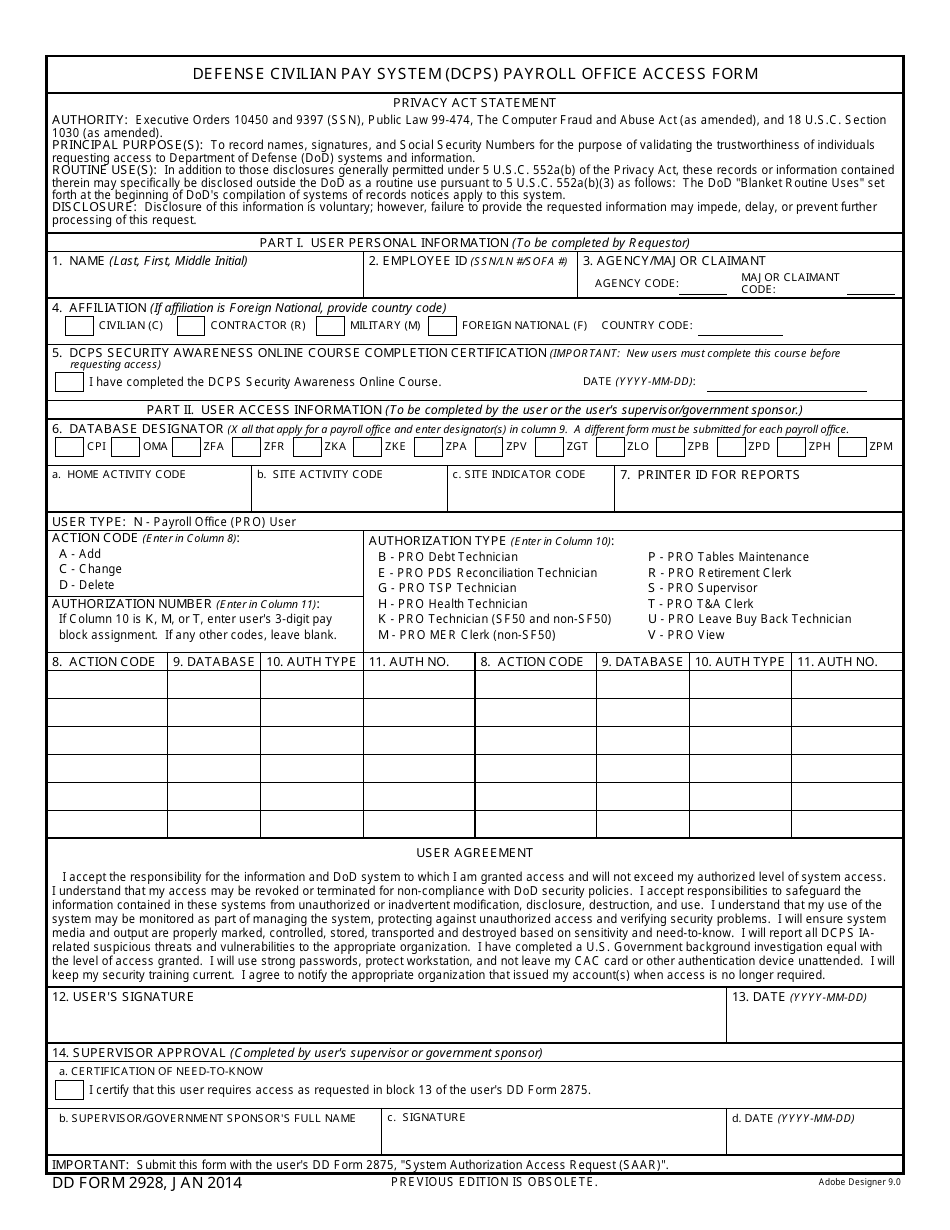
DD Form 2928 Download Fillable PDF or Fill Online Defense Civilian Pay
For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Get everything done in minutes. The dental provider should complete part 2. Please complete all sections including child’s race or ethnicity. As outlined below, a series of medical forms should be turned in to the school as part of the enrollment process, and any updated forms throughout.
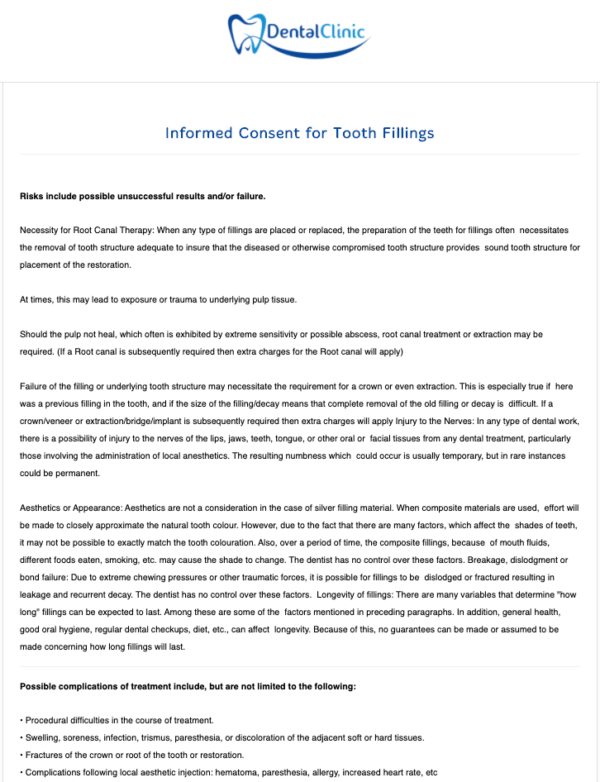
Tooth Fillings Consent Form Dental Form Templates by iPEGS Ltd
Web to choose the plan that fits you best, you may review the health benefits plan summary. All employees are eligible for dental and vision options outlined in the dental/optical section below. Amharic (አማርኛ) (link is external) chinese (中文) (link is external) english. Get everything done in minutes. Child’s clinical examination (to be completed by the dental provider)date of exam.
FREE 28+ Sample Clearance Forms in PDF Ms Word
Please indicate the ward of your home address, list primary care provider, dental provider, and type of dental insurance. Student information (to be completed by parent/guardian) Web universal health certificate use this form to report your child’s physical health to their school/child care facility. Please complete all sections including child’s race or ethnicity. Amharic (አማርኛ) (link is external) chinese (中文).

Dental Exam Form (100/Package)
Get everything done in minutes. Web district of columbia oral health (dental provider) assessment form part 1. Child’s clinical examination (to be completed by the dental provider)date of exam __________________________ (please use key to document all findings on line next to each tooth) For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Child’s personal information part.
Dcps Community Service Form Fill Online, Printable, Fillable, Blank
Amharic (አማርኛ) (link is external) chinese (中文) (link is external) english. Please indicate the ward of your home address, list primary care provider, dental provider, and type of dental insurance. Web health physicals and oral health assessments are required annually. Web to choose the plan that fits you best, you may review the health benefits plan summary. For additional information.
FREE 28+ Sample Clearance Forms in PDF Ms Word
Child’s clinical examination (to be completed by the dental provider)date of exam __________________________ (please use key to document all findings on line next to each tooth) Please complete all sections including child’s race or ethnicity. For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Web district of columbia oral health (dental provider) assessment form parent/guardian instructions:.

Medical Assisting Robert Educational Center & Technical College
Schools must verify every student’s immunization compliance as part of enrollment and attendance (see the school immunization policy for more details). Take this form to the student's dental provider. Web instructions • complete part 1 below. Please indicate the ward of your home address, list primary care provider, dental provider, and type of dental insurance. Web to choose the plan.
DCPS Application to Use Facilities Does Dc Fill Out and Sign
The dental provider should complete part 2. Get everything done in minutes. Child’s personal information part 2. For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Take this form to the student's dental provider.
• Return Fully Completed And Signed Form To The Student's School/Child Care Facility.
The dental provider should complete part 2. Amharic (አማርኛ) (link is external) chinese (中文) (link is external) english. Web district of columbia oral health (dental provider) assessment form part 1. Web district of columbia oral health (dental provider) assessment form parent/guardian instructions:
Please Complete All Sections Including Child’s Race Or Ethnicity.
As outlined below, a series of medical forms should be turned in to the school as part of the enrollment process, and any updated forms throughout the school year should be submitted to the school nurse. Take this form to the student's dental provider. Student information (to be completed by parent/guardian) If the child has no dental provider and is uninsured,
Check Out How Easy It Is To Complete And Esign Documents Online Using Fillable Templates And A Powerful Editor.
Students also must be current with their immunizations to attend school. Part 1:please complete all sections including child’s race or ethnicity. Child’s clinical examination (to be completed by the dental provider)date of exam __________________________ (please use key to document all findings on line next to each tooth) Child’s personal information part 2.
Web Universal Health Certificate Use This Form To Report Your Child’s Physical Health To Their School/Child Care Facility.
Web health physicals and oral health assessments are required annually. Schools must verify every student’s immunization compliance as part of enrollment and attendance (see the school immunization policy for more details). For additional information regarding health benefits, please contact our benefits team at dcps.benefits@k12.dc.gov. Please indicate the ward of your home address, list primary care provider, dental provider, and type of dental insurance.