Davis Vision Claim Form Out Of Network
Davis Vision Claim Form Out Of Network - Vision care processing unit, p.o. What is your position on telehealth services? When filled out, please send them to us by emailing lbs@versanthealth.com. The completion and submission of this form does not guarantee eligibility for benefits. Expenses for both examinations and eyewear can be claimed on this form. If another insurance company is involved, check the box and attach a copy of the statement showing payment. Web please download the below documents. Web davis vision has been providing comprehensive vision care benefits for over 50 years. Client / group name the request is regarding letter of authorization from client / group effective date broker name broker address Enter the amount charged for each applicable line item.
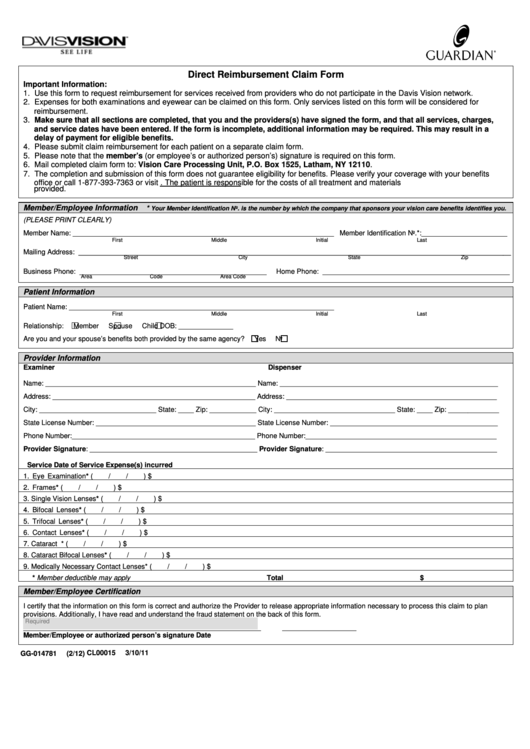
Expenses for both examinations and eyewear can be listed on this form. When filled out, please send them to us by emailing lbs@versanthealth.com. Use this form to request reimbursement for services received from providers not in the davis vision network. Enter the date of service in the following format: Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Vision care processing unit, p.o. Web mail completed claim form to: Only one patient’s services may be claimed on this form. Enter the amount charged for each applicable line item.
When filled out, please send them to us by emailing lbs@versanthealth.com. The completion and submission of this form does not guarantee eligibility for benefits. Vision care processing unit, p.o. Enter the amount charged for each applicable line item. Web mail completed claim form to: Web please download the below documents. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for services received from providers not in the davis vision network. Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. Ensure they match the receipts.

New York State Vision Plan Student Verification Form Fraud Crimes
Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. If another insurance company is involved, check the box and attach a copy of the statement showing payment. Only one patient’s services may be claimed on this form. What is your position on telehealth services? When filled out, please.

Davis Vision Insurance Providers In My Area Does Costco Accept Davis
Only one patient’s services may be claimed on this form. Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. Can members receive care from the eye care professional of their choice? The completion and submission of this form does not guarantee eligibility for benefits. Web use this form to request.
Top Davis Vision Claim Form Templates Free To Download In PDF Format
Vision care processing unit, p.o. Expenses for both examinations and eyewear can be claimed on this form. Can members receive care from the eye care professional of their choice? Ensure they match the receipts. Each patient’s services must be claimed on a separate form.

Davis Vision Moves 100 Jobs to Texas Plainview, NY Patch
Client / group name the request is regarding letter of authorization from client / group effective date broker name broker address Vision care processing unit, p.o. Use this form to request reimbursement for services received from providers not in the davis vision network. Expenses for both examinations and eyewear can be claimed on this form. Enter the date of service.

Davis Vision Android Apps on Google Play
Enter the amount charged for each applicable line item. Each patient’s services must be claimed on a separate form. Ensure they match the receipts. When filled out, please send them to us by emailing lbs@versanthealth.com. Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form.

Claim Form Davis Vision Claim Form
The completion and submission of this form does not guarantee eligibility for benefits. When filled out, please send them to us by emailing lbs@versanthealth.com. Ensure they match the receipts. Web davis vision has been providing comprehensive vision care benefits for over 50 years. Do members need a claim form for services?

Davis Vision for Android APK Download
The completion and submission of this form does not guarantee eligibility for benefits. Enter the date of service in the following format: Each patient’s services must be claimed on a separate form. Expenses for both examinations and eyewear can be claimed on this form. Ensure they match the receipts.
Life Insurance Provider Photos
Use this form to request reimbursement for services received from providers not in the davis vision network. Web davis vision has been providing comprehensive vision care benefits for over 50 years. Enter the date of service in the following format: Log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. If.

Davis Vision Insurance Providers In My Area Does Costco Accept Davis
When filled out, please send them to us by emailing lbs@versanthealth.com. Web davis vision has been providing comprehensive vision care benefits for over 50 years. Ensure they match the receipts. Expenses for both examinations and eyewear can be claimed on this form. Only one patient’s services may be claimed on this form.

Davis Vision Insurance Providers In My Area Does Costco Accept Davis
Web mail completed claim form to: Expenses for both examinations and eyewear can be claimed on this form. Vision care processing unit, p.o. Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Ensure they match the receipts.
Each Patient’s Services Must Be Claimed On A Separate Form.
Can members receive care from the eye care professional of their choice? Enter the date of service in the following format: Web mail completed claim form to: Web use this form to request reimbursement for services received from providers who do not participate in the davis vision network.
The Completion And Submission Of This Form Does Not Guarantee Eligibility For Benefits.
Client / group name the request is regarding letter of authorization from client / group effective date broker name broker address Expenses for both examinations and eyewear can be listed on this form. Enter the amount charged for each applicable line item. Web davis vision has been providing comprehensive vision care benefits for over 50 years.
Log In To Your Account And Click On “Access Benefits And Forms” To Download The Direct Reimbursement Claim Form.
Box 1525, latham, ny 12110. Use this form to request reimbursement for services received from providers not in the davis vision network. Do members need a claim form for services? Web please download the below documents.
Expenses For Both Examinations And Eyewear Can Be Claimed On This Form.
Only one patient’s services may be claimed on this form. Ensure they match the receipts. If another insurance company is involved, check the box and attach a copy of the statement showing payment. When filled out, please send them to us by emailing lbs@versanthealth.com.