Wellmark Appeal Form
Wellmark Appeal Form - Privacy office, mail station 5w590. Web this form is used to authorize wellmark to disclose protected health information at the request of the individual. Claim reconsideration request form [pdf] continuation of. Find individual and family plans and resources for employers, providers, and producers. Utilize the instruments we provide to fill out your form. Web easily find and download forms, questionnaires and other documentation you need to do business with wellmark in one, convenient location. Protected health information form must be. Web if you are requesting an appeal on behalf of the member, a personal representative appointment and authorized to realese. Web if you don't have a consent form, we have created a template you may use. Web better care management better healthcare outcomes.
Web if you are requesting an appeal on behalf of the member, a personal representative appointment and authorized to realese. Web you also agree to limit your access to and use of phi to the minimum necessary to perform an authorized function or inquiry related to treatment, payment or health care operations. Web wellmark makes a decision: The registration form may be used to request a submitter number for submitting electronic claims using create & submit or to add a provider to an. Privacy office, mail station 5w590. Web this form is used to authorize wellmark to disclose protected health information at the request of the individual. The back of your id card states whether you are insured through wellmark bcbs of iowa, wellmark health plan of iowa, or wellmark bcbs of south dakota. Appeal from the district court for polk county. Web send completed and signed form to: You make a difference in your patient's healthcare.
Utilize the instruments we provide to fill out your form. Web if you don't have a consent form, we have created a template you may use. You make a difference in your patient's healthcare. Privacy office, mail station 5w590. Highlight relevant paragraphs of your documents or blackout. Get form discrimination is against the law wellmark complies with. Web send completed and signed form to: Web better care management better healthcare outcomes. To view authorizations and quantity limits for drugs and medications, please view the drug. Web find wellmark appeal form and click get form to get started.
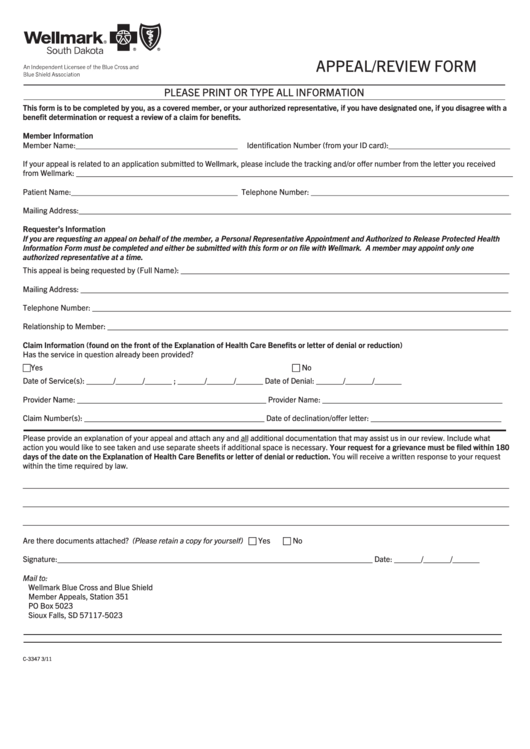
Appeal/review Form Wellmark, South Dakota printable pdf download
Web find wellmark appeal form and click get form to get started. Web wellmark is the leading health insurance company in iowa and south dakota. Highlight relevant paragraphs of your documents or blackout. You will be notified by mail or email of the decision or view the authorization in mywellmark within 24 hours of the decision being made. The back.
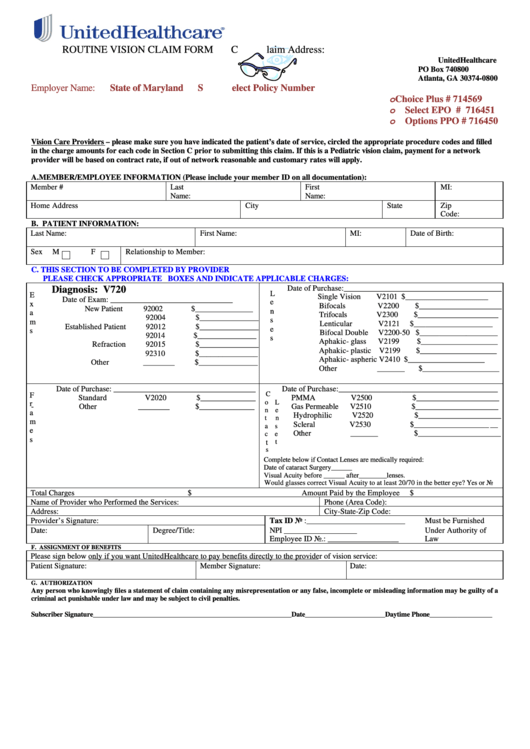
United Healthcare Routine Vision Claim Form printable pdf download
You will be notified by mail or email of the decision or view the authorization in mywellmark within 24 hours of the decision being made. The registration form may be used to request a submitter number for submitting electronic claims using create & submit or to add a provider to an. Web if you don't have a consent form, we.

Free Highmark Prior (Rx) Authorization Form PDF eForms
Find individual and family plans and resources for employers, providers, and producers. Web if you are requesting an appeal on behalf of the member, a personal representative appointment and authorized to realese. We help supply the tools to make a difference. Submit a corrected electronic claim do not submit a corrected electronic. Web easily find and download forms, questionnaires and.

CMS 1500 Forms and Envelopes StockChecks
The registration form may be used to request a submitter number for submitting electronic claims using create & submit or to add a provider to an. Web wellmark is the leading health insurance company in iowa and south dakota. Web wellmark makes a decision: Web you also agree to limit your access to and use of phi to the minimum.
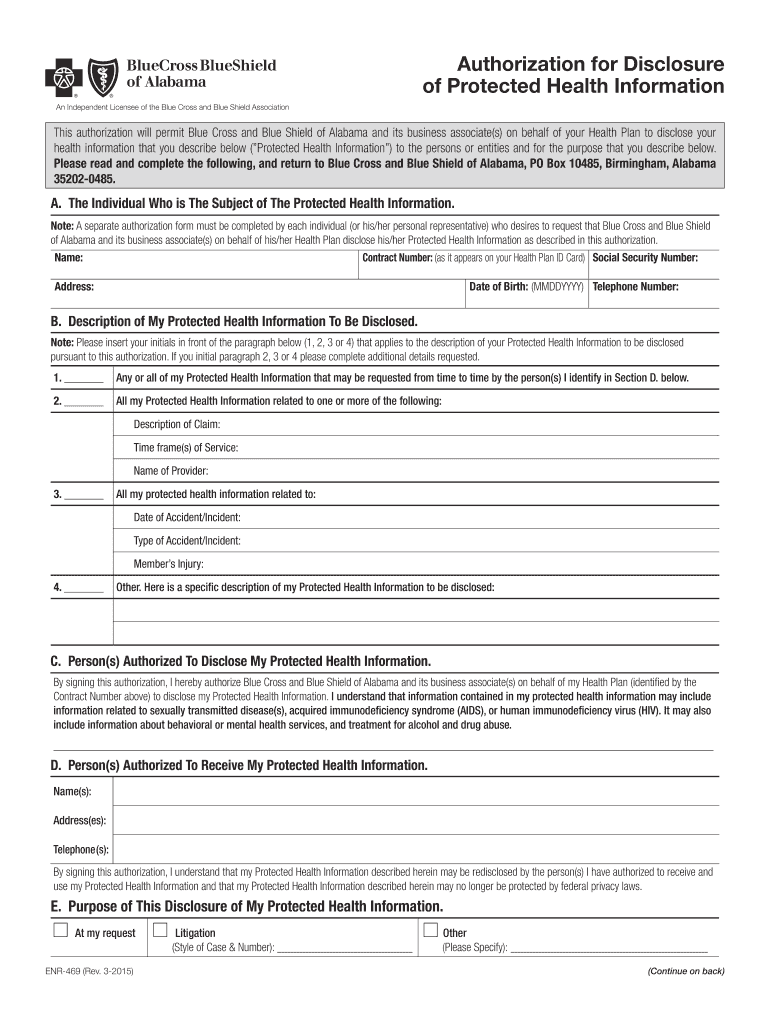
20152022 AL BCBS Form ENR469 Fill Online, Printable, Fillable, Blank
Web authorization form for clinic/group billing [pdf] use for notification that a practitioner is joining a clinic or group. Web this form is used to authorize wellmark to disclose protected health information at the request of the individual. Get form discrimination is against the law wellmark complies with. The registration form may be used to request a submitter number for.
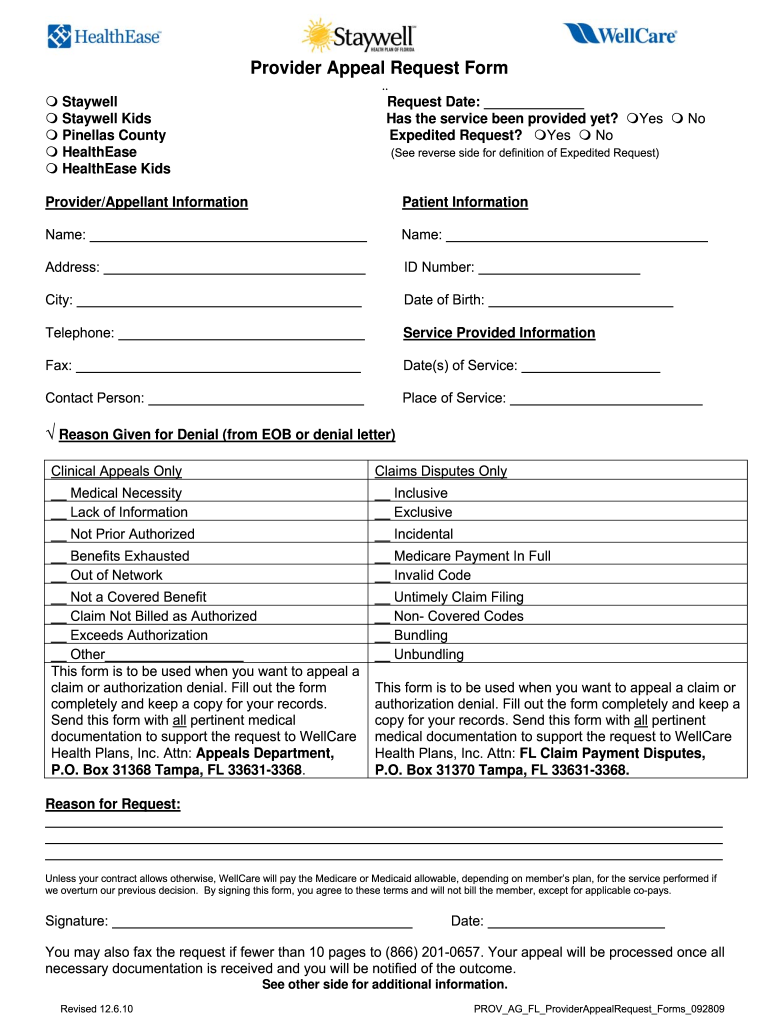
Wellcare Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
Web wellmark makes a decision: Highlight relevant paragraphs of your documents or blackout. Web find wellmark appeal form and click get form to get started. We help supply the tools to make a difference. You make a difference in your patient's healthcare.
letter code Student Appeal Letter Sample
Web easily find and download forms, questionnaires and other documentation you need to do business with wellmark in one, convenient location. You make a difference in your patient's healthcare. Protected health information form must be. To view authorizations and quantity limits for drugs and medications, please view the drug. Privacy office, mail station 5w590.

Ky Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
Web send completed and signed form to: Web this form is used to authorize wellmark to disclose protected health information at the request of the individual. Web find wellmark appeal form and click get form to get started. Privacy office, mail station 5w590. Web use a wellmark provider appeal form template to make your document workflow more streamlined.
Form 1 Download Fillable PDF or Fill Online Notice of Appeal
Get form discrimination is against the law wellmark complies with. Highlight relevant paragraphs of your documents or blackout. Web better care management better healthcare outcomes. Web wellmark is the leading health insurance company in iowa and south dakota. Utilize the instruments we provide to fill out your form.

IA Wellmark BCBS P4602 20202021 Fill and Sign Printable Template
Find individual and family plans and resources for employers, providers, and producers. The back of your id card states whether you are insured through wellmark bcbs of iowa, wellmark health plan of iowa, or wellmark bcbs of south dakota. Web this form is used to authorize wellmark to disclose protected health information at the request of the individual. Web if.
Web Wellmark Is The Leading Health Insurance Company In Iowa And South Dakota.
Claim reconsideration request form [pdf] continuation of. Protected health information form must be. Web you also agree to limit your access to and use of phi to the minimum necessary to perform an authorized function or inquiry related to treatment, payment or health care operations. Web if you don't have a consent form, we have created a template you may use.
Web Send Completed And Signed Form To:
Web better care management better healthcare outcomes. We help supply the tools to make a difference. Web if you are requesting an appeal on behalf of the member, a personal representative appointment and authorized to realese. You make a difference in your patient's healthcare.
Find Individual And Family Plans And Resources For Employers, Providers, And Producers.
Appeal from the district court for polk county. Web easily find and download forms, questionnaires and other documentation you need to do business with wellmark in one, convenient location. Privacy office, mail station 5w590. Web this form is used to authorize wellmark to disclose protected health information at the request of the individual.
Get Form Discrimination Is Against The Law Wellmark Complies With.
You will be notified by mail or email of the decision or view the authorization in mywellmark within 24 hours of the decision being made. Wellmark blue cross and blue shield. Web find wellmark appeal form and click get form to get started. To view authorizations and quantity limits for drugs and medications, please view the drug.