Wc-36 Form
Wc-36 Form - Web state of hawaii department of labor and industrial relations disability compensation division p.o. Web division of workers’ compensation. Web wc 36 form hawaii. Must be accompanied by a. Web the form 36 is to be completed by the respondent (employer/workers’ compensation insurance carrier) to notify the workers’ compensation commissioner, the. Web the form 36 is to be completed by the respondent (employer/workers’ compensation insurance carrier) to notify the workers’ compensation commissioner, the. The document is addressed to the sheriff of the applicable county. Box 3769 honolulu, hawaii 96812 phone: Signature of person authorized to sign for employer phone number. Web the form 36 is to be completed by the respondent (employer/workers' compensation insurance carrier) to notify the workers' compensation commissioner, the claimant.
Form 42, application for appointment of guardian ad litem; Web the form 36 is to be completed by the respondent (employer/workers’ compensation insurance carrier) to notify the workers’ compensation commissioner, the. Web get the latest workers' compensation insurance forms for hawaii. Web state of hawaii department of labor and industrial relations disability compensation division p.o. Edit, esign, and send out your wc 36 form hawaii from signnow. Substitution of attorneys _____ appoints _____ astorney his. Signature of person authorized to sign for employer phone number. The employer must send the form to the claimant. Must be accompanied by a. Form 51, annual consolidated fiscal report of.
Web state of hawaii department of labor and industrial relations disability compensation division p.o. Web state of connecticut workers’ compensation commission you are hereby notified that the employer/insurer intends to reduce or discontinue your compensation. On 12/12/2012 hiwa was granted its non. The employer must send the form to the claimant. Save your time by managing your labor forms online. Web north carolina industrial commission form 36 is a subpoena for witness. Get everything done in minutes. (1) immediately notify your connecticut workers comp attorney who will file an. Web if you receive a form 36 and contend that total incapacity continues, you should: • in the event of a medical emergency, call 911 or follow your agency’s emergency medical.

JETLINE Type WC36Z Welding Chamber
• in the event of a medical emergency, call 911 or follow your agency’s emergency medical. Signature of person authorized to sign for employer phone number. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web north carolina industrial commission form 36 is a subpoena for witness. Web state of.

Form WC126 Download Fillable PDF or Fill Online Authorization to
Form 44, application for review; Must be accompanied by a. Get everything done in minutes. (1) immediately notify your connecticut workers comp attorney who will file an. Web get the latest workers' compensation insurance forms for hawaii.
Form WC132 Download Fillable PDF or Fill Online Electronic Fund
Web if you receive a form 36 and contend that total incapacity continues, you should: The employer must send the form to the claimant. Web form 36, subpoena for witness; Access common workers' comp forms hawaii, applications, guides and helpful manuals for hi. Web the form 36 is to be completed by the respondent (employer/workers' compensation insurance carrier) to notify.
Form 36 Download Fillable PDF or Fill Online Tax Clearance Application
Access common workers' comp forms hawaii, applications, guides and helpful manuals for hi. Form 44, application for review; Box 3769 honolulu, hawaii 96812 phone: Form 42, application for appointment of guardian ad litem; Must be accompanied by a.
Form 10133.36 Download Fillable PDF or Fill Online Physician's Return
Web the form 36 is to be completed by the respondent (employer/workers’ compensation insurance carrier) to notify the workers’ compensation commissioner, the. Web the form 36 is to be completed by the respondent (employer/workers' compensation insurance carrier) to notify the workers' compensation commissioner, the claimant. Must be accompanied by a. Form 51, annual consolidated fiscal report of. Web state of.

JETLINE Type WC36Z Welding Chamber
Web get the latest workers' compensation insurance forms for hawaii. Box 3769 honolulu, hawaii 96812 phone: Save your time by managing your labor forms online. Form 44, application for review; Edit, esign, and send out your wc 36 form hawaii from signnow.

2011 Form GA WC14 Fill Online, Printable, Fillable, Blank pdfFiller
Get everything done in minutes. Signature of person authorized to sign for employer phone number. On 12/12/2012 hiwa was granted its non. Save your time by managing your labor forms online. Web north carolina industrial commission form 36 is a subpoena for witness.
Wc 1 Form Fill Out and Sign Printable PDF Template signNow
Web state of hawaii department of labor and industrial relations disability compensation division p.o. Access common workers' comp forms hawaii, applications, guides and helpful manuals for hi. Get everything done in minutes. Web division of workers’ compensation. Web get the latest workers' compensation insurance forms for hawaii.
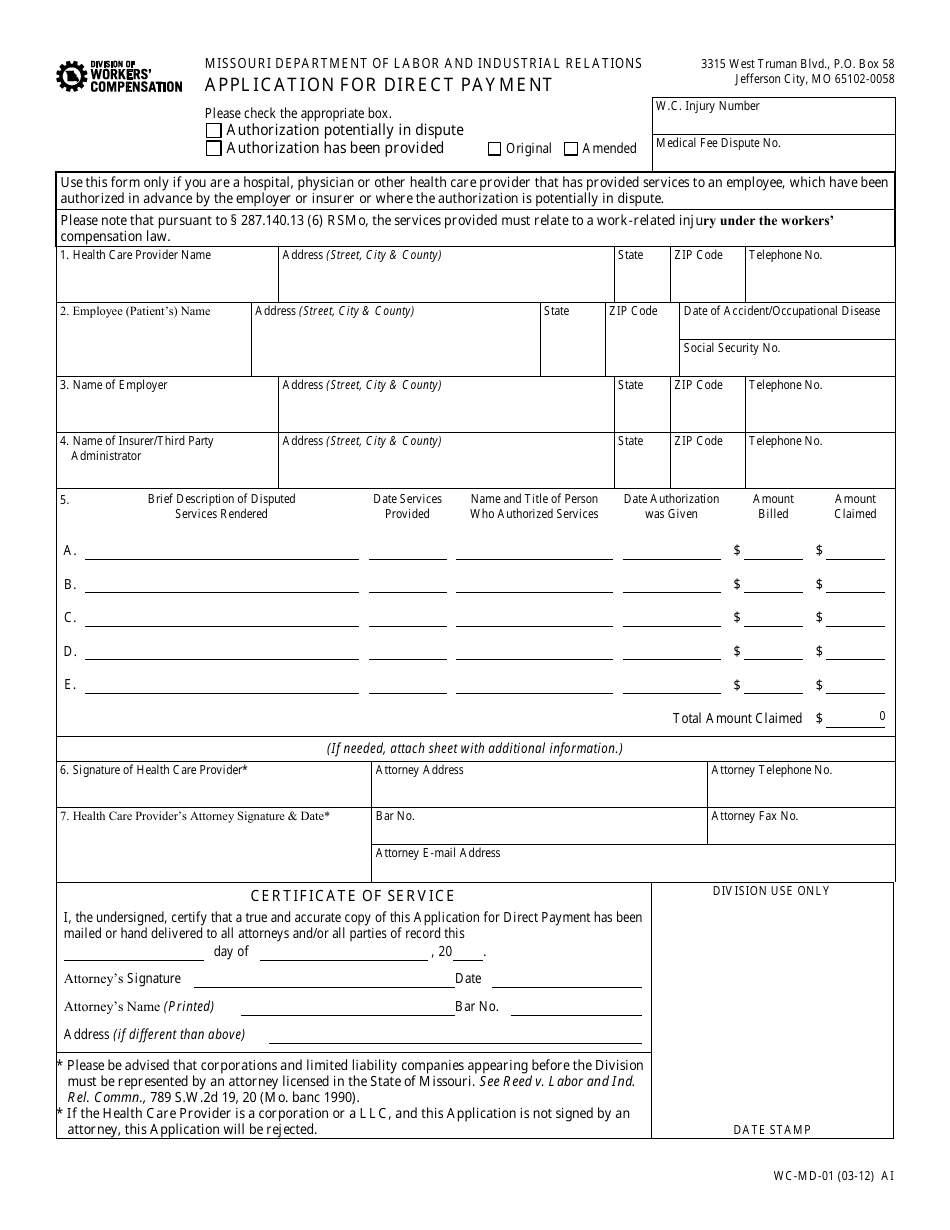
Form WCMD01 Download Fillable PDF or Fill Online Application for
Form 44, application for review; Division of longshore and harbor workers’ compensation by electronic submission via. Web the form 36 is to be completed by the respondent (employer/workers’ compensation insurance carrier) to notify the workers’ compensation commissioner, the. Web to do so, an employer must file a form 36, which is required to be signed by a physician licensed in.

Wc P1 7 2006 Fillable Fill and Sign Printable Template Online US
Web workers' compensation for employees. On 12/12/2012 hiwa was granted its non. Web the form 36 is to be completed by the respondent (employer/workers' compensation insurance carrier) to notify the workers' compensation commissioner, the claimant. Web wc 36 form hawaii. Web state of hawaii department of labor and industrial relations disability compensation division p.o.
The Employer Must Send The Form To The Claimant.
Web north carolina industrial commission form 36 is a subpoena for witness. Web to do so, an employer must file a form 36, which is required to be signed by a physician licensed in connecticut. Box 3769 honolulu, hawaii 96812 phone: On 12/12/2012 hiwa was granted its non.
Check Out How Easy It Is To Complete And Esign Documents Online Using Fillable Templates And A Powerful Editor.
Signature of person authorized to sign for employer phone number. Web form 36, subpoena for witness; Web state of hawaii department of labor and industrial relations disability compensation division p.o. Form 51, annual consolidated fiscal report of.
• In The Event Of A Medical Emergency, Call 911 Or Follow Your Agency’s Emergency Medical.
Get everything done in minutes. The document is addressed to the sheriff of the applicable county. Web wc 36 form hawaii. Save your time by managing your labor forms online.
Division Of Longshore And Harbor Workers’ Compensation By Electronic Submission Via.
(1) immediately notify your connecticut workers comp attorney who will file an. Must be accompanied by a. Web state of connecticut workers’ compensation commission you are hereby notified that the employer/insurer intends to reduce or discontinue your compensation. Web the form 36 is to be completed by the respondent (employer/workers’ compensation insurance carrier) to notify the workers’ compensation commissioner, the.