Tricare 3Rd Party Liability Form
Tricare 3Rd Party Liability Form - The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below. When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Subrogation/lien cases involving third party liability should be. Web check box to indicate if patient's condition is accident related, work related or both. Check your region's forms page if you don't find what. Web if you need to file a claim for care yourself, visit the claims section to access the proper form. Web third party liability claim form (dd2527) send third party liability form to: Web some diagnosis codes can indicate an injury or illness which may have been caused by a third party. Describe condition for which patient received treatment, supplies, or medication Are you looking for another form?
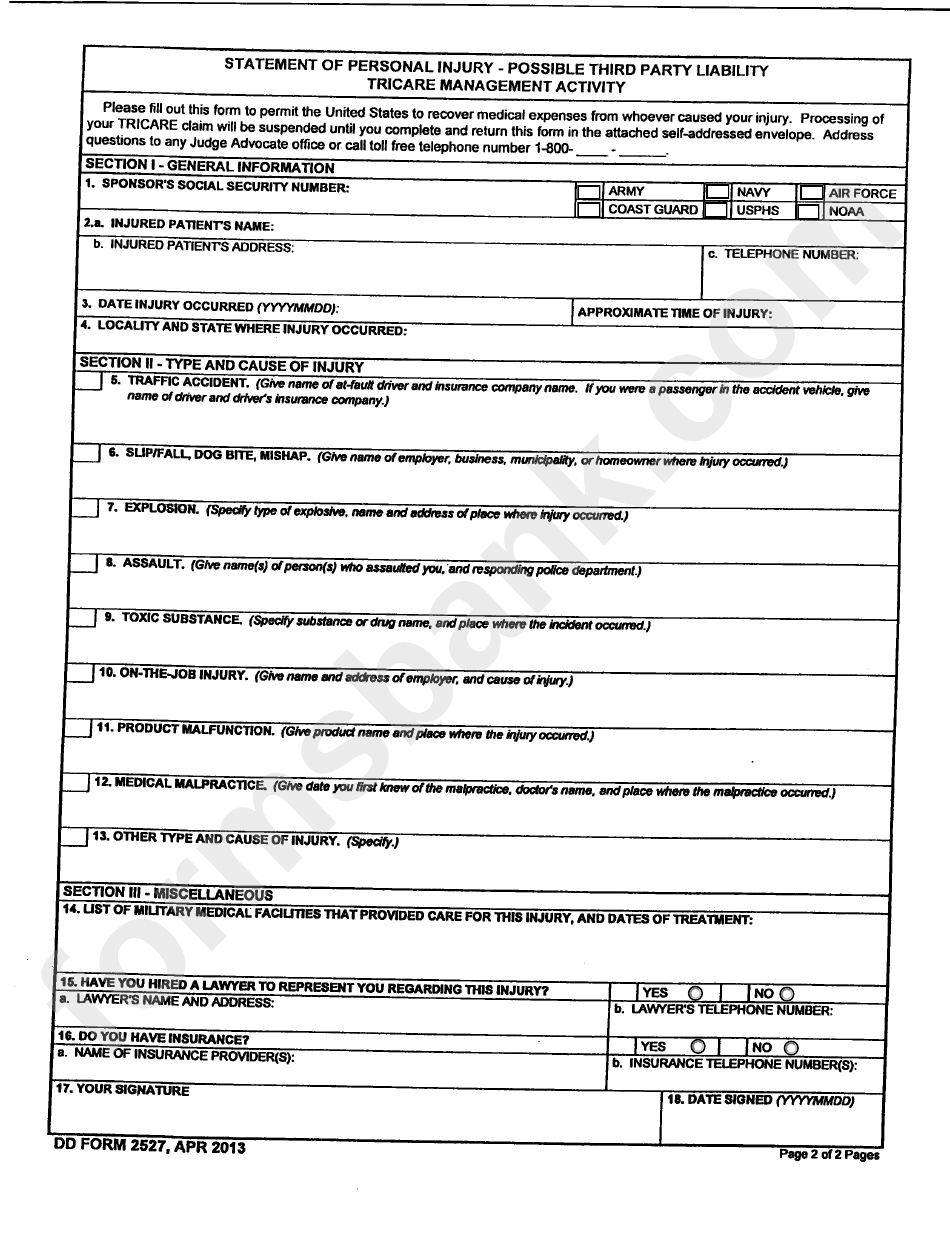
The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below. Subrogation/lien cases involving third party liability should be. Web if you need to file a claim for care yourself, visit the claims section to access the proper form. Web some diagnosis codes may indicate an injury or illness which a third party may have caused. When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Web check box to indicate if patient's condition is accident related, work related or both. Describe condition for which patient received treatment, supplies, or medication Web third party liability claim form (dd2527) send third party liability form to: Check your region's forms page if you don't find what. Are you looking for another form?
When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Web check box to indicate if patient's condition is accident related, work related or both. Check your region's forms page if you don't find what. The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below. Subrogation/lien cases involving third party liability should be. Web some diagnosis codes can indicate an injury or illness which may have been caused by a third party. Web third party liability claim form (dd2527) send third party liability form to: Are you looking for another form? Web if you need to file a claim for care yourself, visit the claims section to access the proper form. Describe condition for which patient received treatment, supplies, or medication
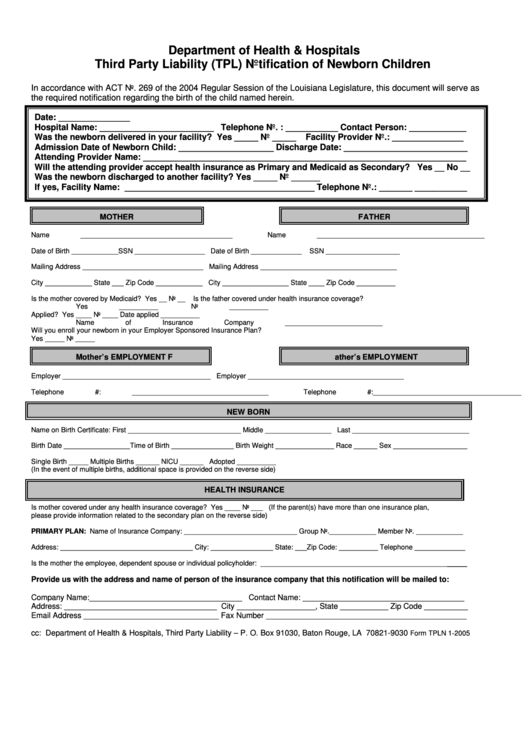
Third Party Liability (Tpl) Notification Of Newborn Children Form
Are you looking for another form? The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below. Web if you need to file a claim for care yourself, visit the claims section to access the proper form. When tricare receives claims with these types of diagnosis codes, we mail the dd2527.
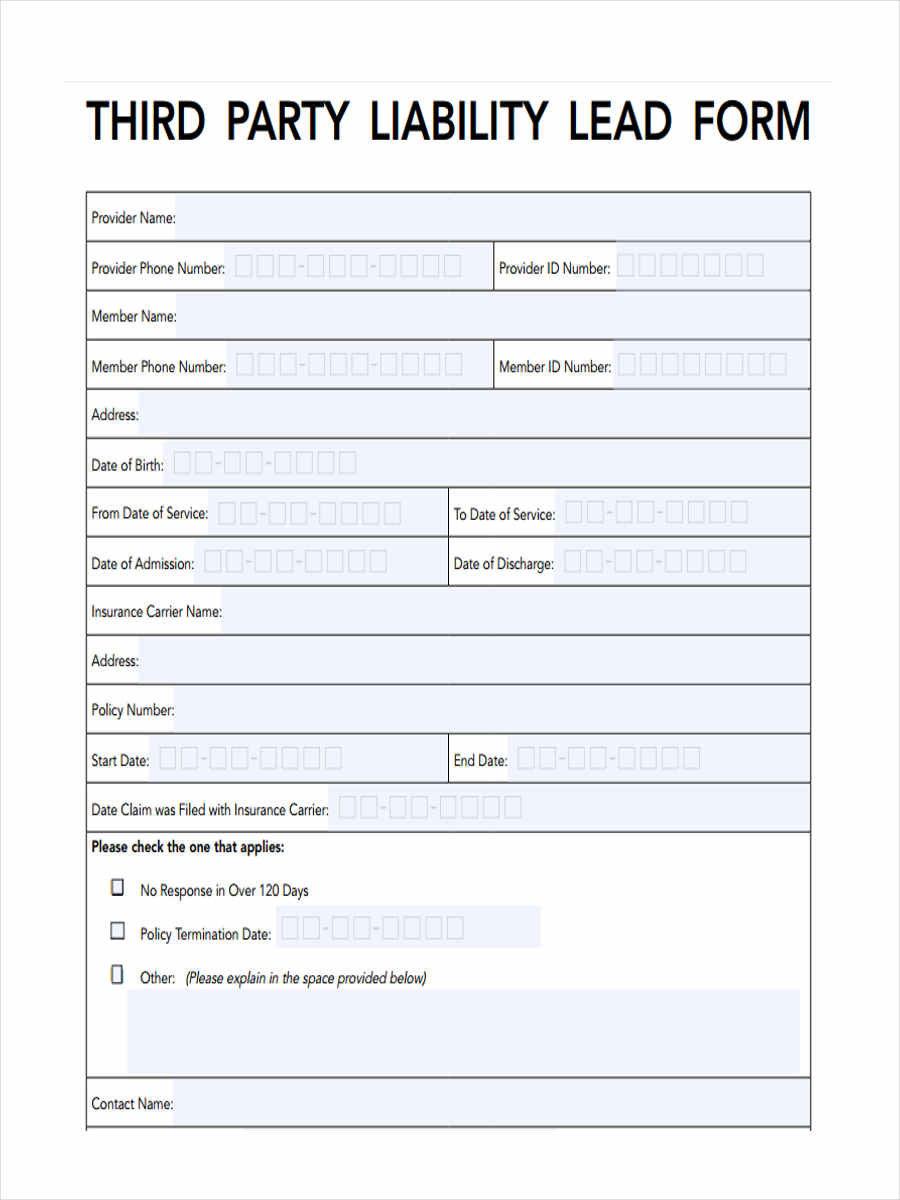
FREE 5+ Third Party Liability Forms in PDF
Web some diagnosis codes may indicate an injury or illness which a third party may have caused. Web third party liability claim form (dd2527) send third party liability form to: Check your region's forms page if you don't find what. When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients.
Fillable Tricare Third Party Liability South Texas Bone & Joint
When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Web some diagnosis codes may indicate an injury or illness which a third party may have caused. Web third party liability claim form (dd2527) send third party liability.
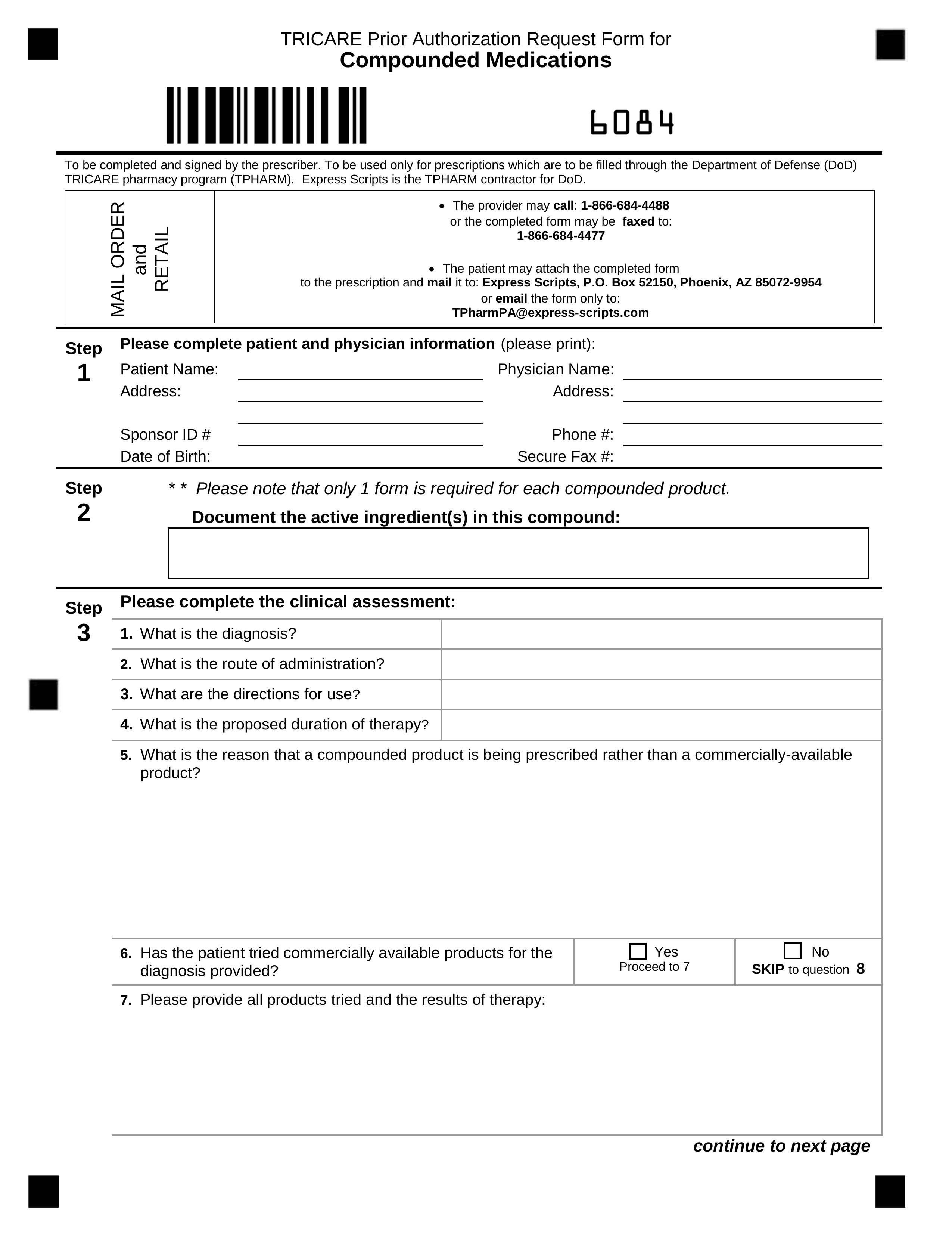
Free TRICARE Prior (Rx) Authorization Form PDF eForms Free
Web third party liability claim form (dd2527) send third party liability form to: Web if you need to file a claim for care yourself, visit the claims section to access the proper form. The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below. When tricare receives claims with these types.
FREE 5+ Third Party Liability Forms in PDF
Describe condition for which patient received treatment, supplies, or medication Web check box to indicate if patient's condition is accident related, work related or both. The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below. Web some diagnosis codes can indicate an injury or illness which may have been caused.
FREE 5+ Third Party Liability Forms in MS Word PDF
Web some diagnosis codes can indicate an injury or illness which may have been caused by a third party. Are you looking for another form? Subrogation/lien cases involving third party liability should be. Check your region's forms page if you don't find what. When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability.

In what may be the latest version of blameshifting, Express Scripts
Web some diagnosis codes can indicate an injury or illness which may have been caused by a third party. The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below. When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or.

Does TRICARE Cover Addiction Treatment? Canyon Crossing Recovery
When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Describe condition for which patient received treatment, supplies, or medication Subrogation/lien cases involving third party liability should be. Are you looking for another form? Web third party liability.

Humana Waiver Of Liability Form Http Resourcebrokerage Com Humana
Web third party liability claim form (dd2527) send third party liability form to: Subrogation/lien cases involving third party liability should be. When tricare receives claims with these types of diagnosis codes, we mail the dd2527 third party liability form to patients or sponsors in order to determine how the injury or illness occurred. Web check box to indicate if patient's.
FREE 5+ Third Party Liability Forms in MS Word PDF
Check your region's forms page if you don't find what. Web check box to indicate if patient's condition is accident related, work related or both. Subrogation/lien cases involving third party liability should be. Web some diagnosis codes can indicate an injury or illness which may have been caused by a third party. When tricare receives claims with these types of.
Web Third Party Liability Claim Form (Dd2527) Send Third Party Liability Form To:
Subrogation/lien cases involving third party liability should be. Web check box to indicate if patient's condition is accident related, work related or both. Are you looking for another form? Web if you need to file a claim for care yourself, visit the claims section to access the proper form.
Web Some Diagnosis Codes May Indicate An Injury Or Illness Which A Third Party May Have Caused.
Web some diagnosis codes can indicate an injury or illness which may have been caused by a third party. Check your region's forms page if you don't find what. Describe condition for which patient received treatment, supplies, or medication The beneficiary must complete and sign this form within 35 calendar days and return the form to the address below.