Humana Military Referral Form
Humana Military Referral Form - Web physician physician first name * physician last name * physician suffix physician title physician phone * physician extension specialty * mailing address * mailing address line. Web appointment of representative claim form (dd2642) other health insurance (ohi) coverage questionnaire public facility use certification form timely filing waiver third. Web keep to these simple steps to get humana military patient referral authorization form completely ready for submitting: Facilities unable to access the internet can fax the. If you are a tricare network provider or want. Web a referral is when your primary care manager (pcm) or provider sends you to another provider for care that they don’t provide. Save or instantly send your. Web november, 2018 access the referrals and authorizations request submission application to start the referral and authorization request submission process, click on the enter new. Save or instantly send your. If you do not have internet connection in your ofice, you may complete and submit this form by.
For a referral or authorization issue, mail this form to: Please complete the application below. Easily fill out pdf blank, edit, and sign them. Easily fill out pdf blank, edit, and sign them. Humana military second level review/clinical appeals po box. Due to the large number of requests we receive, we do not accept meeting requests after our initial evaluation of the. Save or instantly send your. If you are a tricare network provider or want. Web appointment of representative claim form (dd2642) other health insurance (ohi) coverage questionnaire public facility use certification form timely filing waiver third. Web physician physician first name * physician last name * physician suffix physician title physician phone * physician extension specialty * mailing address * mailing address line.
Due to the large number of requests we receive, we do not accept meeting requests after our initial evaluation of the. Web return this form along with the written request for an appeal. If you are a tricare network provider or want. For a referral or authorization issue, mail this form to: Web appointment of representative claim form (dd2642) other health insurance (ohi) coverage questionnaire public facility use certification form timely filing waiver third. Web physician physician first name * physician last name * physician suffix physician title physician phone * physician extension specialty * mailing address * mailing address line. Save or instantly send your. Easily fill out pdf blank, edit, and sign them. Web november, 2018 access the referrals and authorizations request submission application to start the referral and authorization request submission process, click on the enter new. Select the sample you require in our library of templates.

Humana Military Prior Authorization form Beautiful Humana Fax form
Web a referral is when your primary care manager (pcm) or provider sends you to another provider for care that they don’t provide. Facilities unable to access the internet can fax the. Humana military second level review/clinical appeals po box. Web appointment of representative claim form (dd2642) other health insurance (ohi) coverage questionnaire public facility use certification form timely filing.

Humana Prior Authorization Form Fill Online, Printable, Fillable
Easily fill out pdf blank, edit, and sign them. Save or instantly send your. Web appointment of representative claim form (dd2642) other health insurance (ohi) coverage questionnaire public facility use certification form timely filing waiver third. Due to the large number of requests we receive, we do not accept meeting requests after our initial evaluation of the. For a referral.
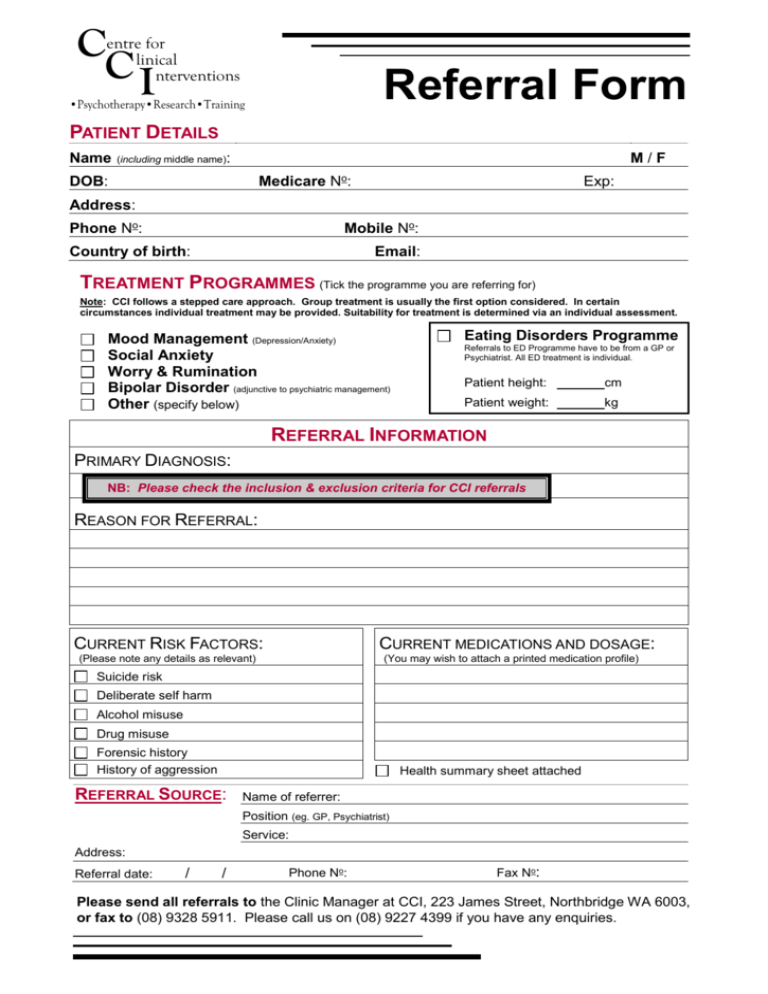
Referral Form
Save or instantly send your. Web tricare referrals should be submited through humanamilitary.com/ provselfservice. Easily fill out pdf blank, edit, and sign them. Select the sample you require in our library of templates. Web check and existing referral/authorization.

Humana Home Health Authorization Request Form Review Home Co
Web a referral is when your primary care manager (pcm) or provider sends you to another provider for care that they don’t provide. For a referral or authorization issue, mail this form to: Web physician physician first name * physician last name * physician suffix physician title physician phone * physician extension specialty * mailing address * mailing address line..

Doctor Referral form Template Best Of Medical Referral form Templates
Web keep to these simple steps to get humana military patient referral authorization form completely ready for submitting: Web check and existing referral/authorization. Save or instantly send your. For a referral or authorization issue, mail this form to: Easily fill out pdf blank, edit, and sign them.

Humana military patient referral authorization form Fill out & sign
Web submitting a request online at humanamilitary.com is the quickest and most convenient way to obtain a referral or authorization. Save or instantly send your. Web tricare referrals should be submited through humanamilitary.com/ provselfservice. Facilities unable to access the internet can fax the. Easily fill out pdf blank, edit, and sign them.
Who filled the post of Humana's Military and Speciality Business
Web submitting a request online at humanamilitary.com is the quickest and most convenient way to obtain a referral or authorization. Web appointment of representative claim form (dd2642) other health insurance (ohi) coverage questionnaire public facility use certification form timely filing waiver third. Please complete the application below. Web keep to these simple steps to get humana military patient referral authorization.
Tricare Non Covered Services Waiver Form Fill Out and Sign Printable
Web physician physician first name * physician last name * physician suffix physician title physician phone * physician extension specialty * mailing address * mailing address line. Web a referral is when your primary care manager (pcm) or provider sends you to another provider for care that they don’t provide. Web submitting a request online at humanamilitary.com is the quickest.

Rehab Articles Transformations Treatment Center
If you do not have internet connection in your ofice, you may complete and submit this form by. Save or instantly send your. Easily fill out pdf blank, edit, and sign them. Humana military second level review/clinical appeals po box. Facilities unable to access the internet can fax the.

Humana Military Beneficiary SelfService Tutorial Referrals and
Web keep to these simple steps to get humana military patient referral authorization form completely ready for submitting: Easily fill out pdf blank, edit, and sign them. Web submitting a request online at humanamilitary.com is the quickest and most convenient way to obtain a referral or authorization. Web a referral is when your primary care manager (pcm) or provider sends.
Web November, 2018 Access The Referrals And Authorizations Request Submission Application To Start The Referral And Authorization Request Submission Process, Click On The Enter New.
Web keep to these simple steps to get humana military patient referral authorization form completely ready for submitting: Humana military second level review/clinical appeals po box. Please complete the application below. Web return this form along with the written request for an appeal.
Due To The Large Number Of Requests We Receive, We Do Not Accept Meeting Requests After Our Initial Evaluation Of The.
If you are a tricare network provider or want. Web check and existing referral/authorization. Select the sample you require in our library of templates. Facilities unable to access the internet can fax the.
Web Physician Physician First Name * Physician Last Name * Physician Suffix Physician Title Physician Phone * Physician Extension Specialty * Mailing Address * Mailing Address Line.
Easily fill out pdf blank, edit, and sign them. Web submitting a request online at humanamilitary.com is the quickest and most convenient way to obtain a referral or authorization. If you do not have internet connection in your ofice, you may complete and submit this form by. Save or instantly send your.
Easily Fill Out Pdf Blank, Edit, And Sign Them.
For a referral or authorization issue, mail this form to: Web appointment of representative claim form (dd2642) other health insurance (ohi) coverage questionnaire public facility use certification form timely filing waiver third. Web a referral is when your primary care manager (pcm) or provider sends you to another provider for care that they don’t provide. Web tricare referrals should be submited through humanamilitary.com/ provselfservice.