Form Dwc 1
Form Dwc 1 - Specifically authorized by section 440.185(2), florida statutes. 6/10 if you are injured or become ill, either physically or. Number workers' compensation claim form. 1/1/2016 page 1 of 3. Web find common forms used during the claims process and throughout your policy period. Employer's report of occupational injury or illness: Full listing of forms and notices by number. Web formulario de reclamo de compensación de trabajadores (dwc 1) y notificación de posible elegibilidad rev. The collection of the social security number on this form is. Claims and return to work.
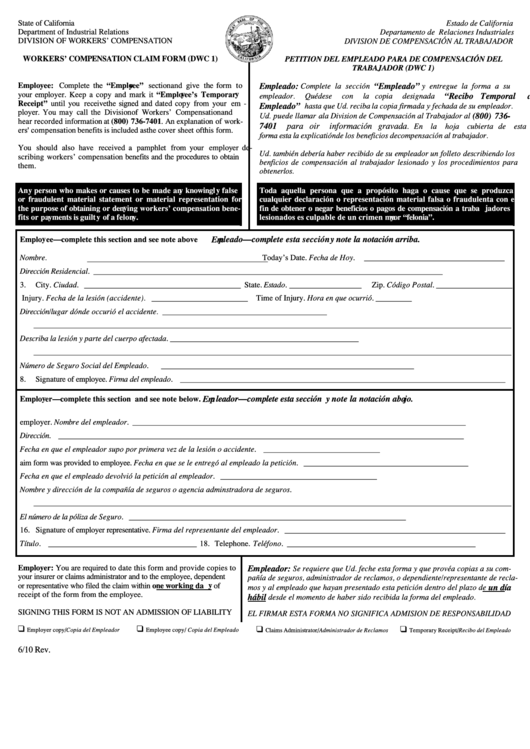
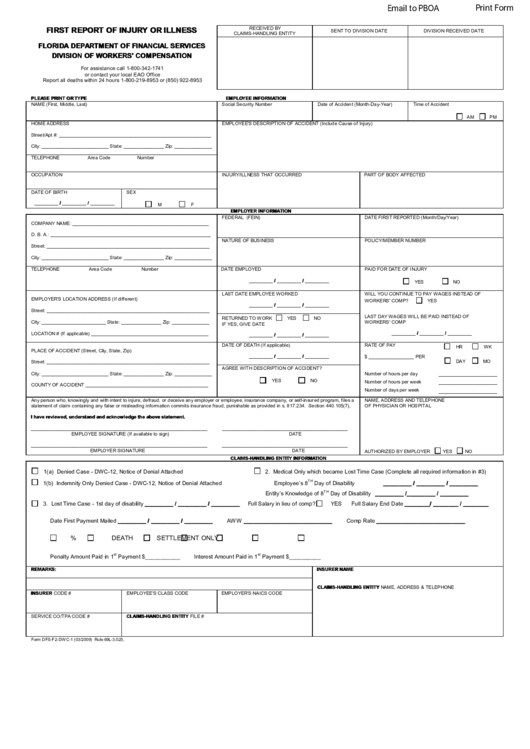
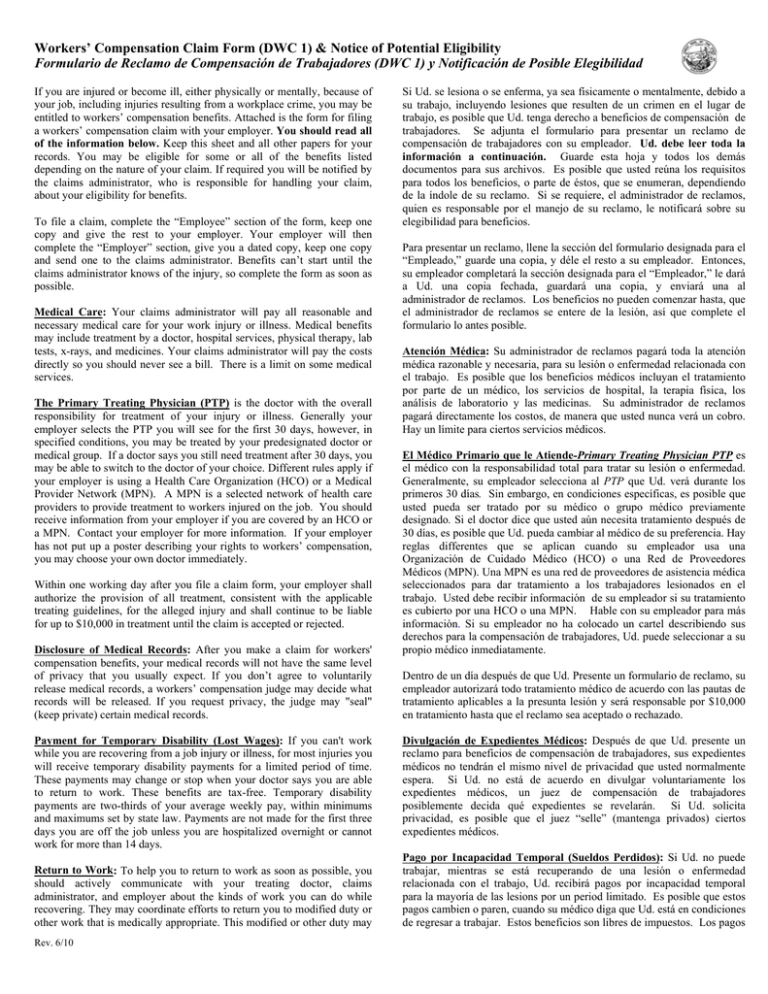
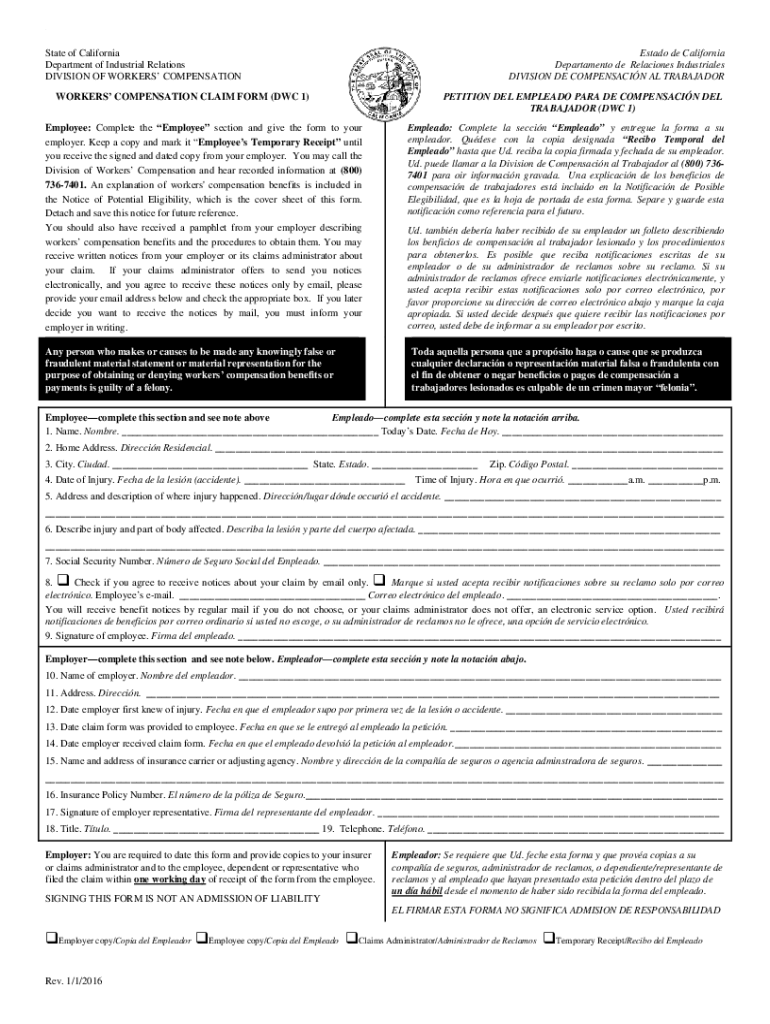
Web formulario de reclamo de compensación de trabajadores (dwc 1) y notificación de posible elegibilidad if you are injured or become ill, either physically or mentally,. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be. Web the employeris required to file an employer's first report of injury or illness. Full listing of forms and notices by number. 6/10 if you are injured or become ill, either physically or. You can obtain a copy of the california dwc 1 claim form here. File a claim form to protect your rights and start the workers’ compensation process. Web formulario de reclamo de compensación de trabajadores (dwc 1) y notificación de posible elegibilidad rev. A dwc 1 is the form that is filled out to report an injury to your employer, and officially initiate a workers’ compensation claim. Claims and return to work.
6/10 if you are injured or become ill, either physically or. How i return to work. File a claim form to protect your rights and start the workers’ compensation process. Web texas department of insurance If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be. How my case is resolved. Web what is a dwc 1 form? 1/1/2016 page 1 of 3. Web formulario de reclamo de compensación de trabajadores (dwc 1) y notificación de posible elegibilidad rev. Give this form to the employee and have them.
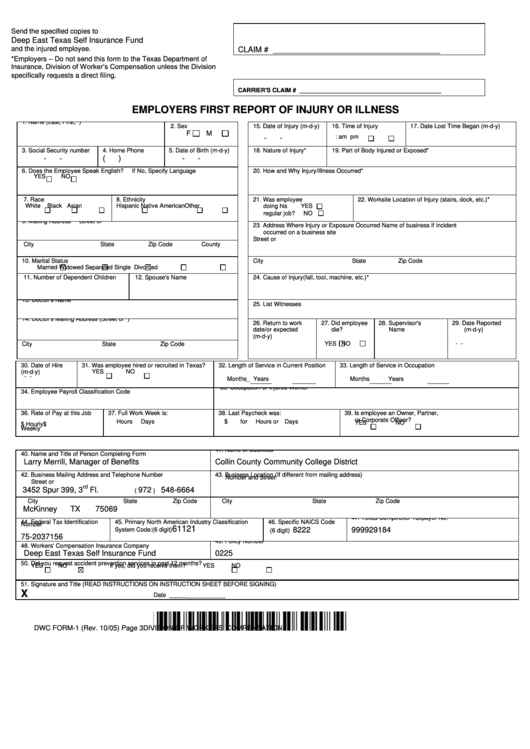
Dwc Form1 Employers First Report Of Injury Or Illness 2005
Number workers' compensation claim form. The collection of the social security number on this form is. Full listing of forms and notices by number. Web what is a dwc 1 form? 1/1/2016 page 1 of 3.

2008 Form CA DWCCA 10232.1 Fill Online, Printable, Fillable, Blank
The collection of the social security number on this form is. Web workers' compensation claim form (dwc 1) & notice of potential eligibility formulario de reclamo de compensación para trabajadores (dwc 1) y notificación de posible. 10/05)] with the injured worker's insurance carrier, and the injured claimant or the. How my case is resolved. How i return to work.
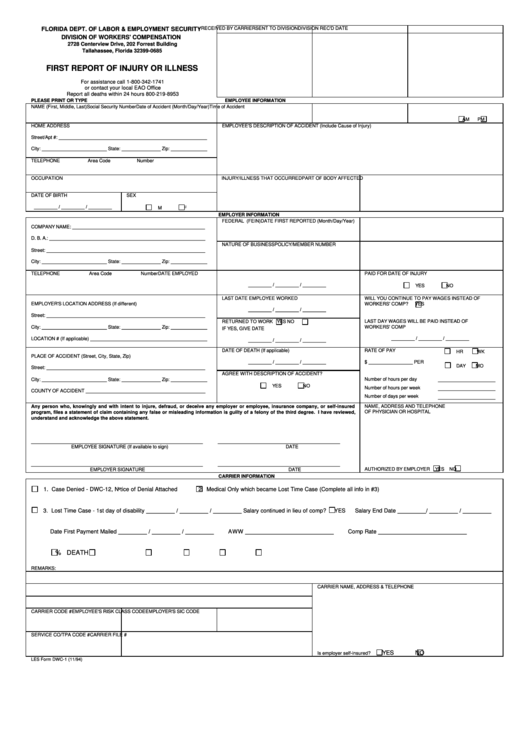
Les Form Dwc1 First Report Of Injury Or Illness Florida Dept. Of
Claims and return to work. Web find common forms used during the claims process and throughout your policy period. 10/05)] with the injured worker's insurance carrier, and the injured claimant or the. How my case is resolved. 1/1/2016 page 1 of 3.
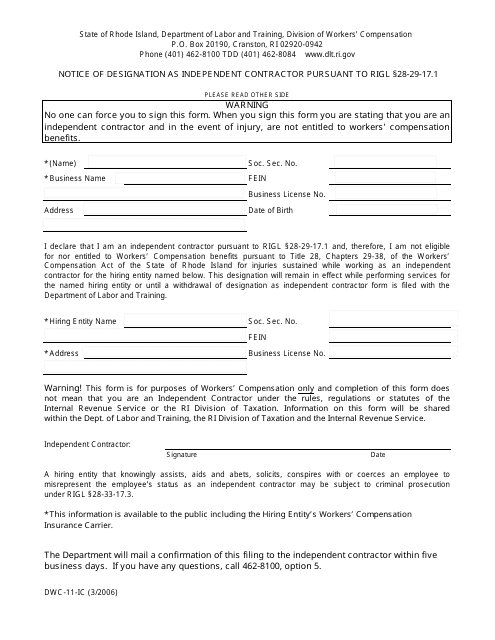
Form DWC11IC Download Fillable PDF or Fill Online Notice of
Web texas department of insurance Specifically authorized by section 440.185(2), florida statutes. Claims and return to work. 10/05)] with the injured worker's insurance carrier, and the injured claimant or the. File a claim form to protect your rights and start the workers’ compensation process.
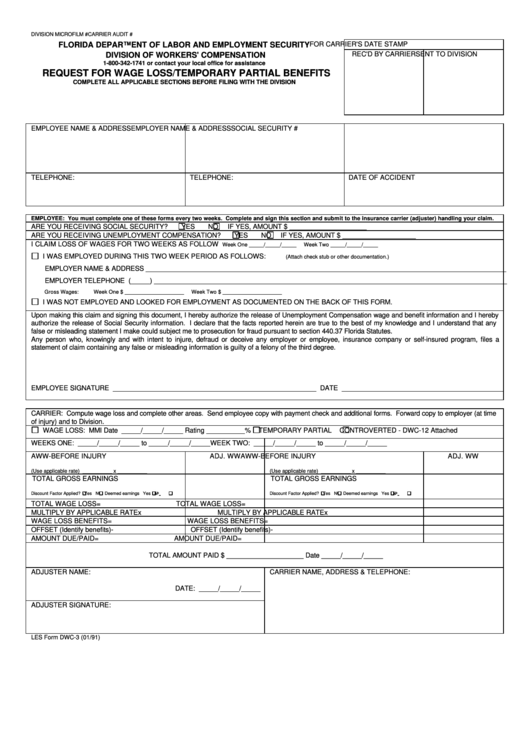
Les Form Dwc3 Request For Wage Loss/temporary Partial Benefits 1991
Full listing of forms and notices by number. Web if my claim was denied. Web what is a dwc 1 form? Web the division of workers' compensation (dwc) monitors the administration of workers' compensation claims, and provides administrative and judicial services to assist in. Employer's report of occupational injury or illness:

Fillable Online Workers' Compensation Claim Form (DWC 1) & Notice of
Web the employeris required to file an employer's first report of injury or illness. Web find common forms used during the claims process and throughout your policy period. File a claim form to protect your rights and start the workers’ compensation process. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting.
Form Dwc 1 Workers' Compensation Claim Form printable pdf download
Web the division of workers' compensation (dwc) monitors the administration of workers' compensation claims, and provides administrative and judicial services to assist in. How i return to work. File a claim form to protect your rights and start the workers’ compensation process. Web texas department of insurance Give this form to the employee and have them.
First Report Of Injury Or Illness Form
10/05)] with the injured worker's insurance carrier, and the injured claimant or the. File a claim form to protect your rights and start the workers’ compensation process. Web the division of workers' compensation (dwc) monitors the administration of workers' compensation claims, and provides administrative and judicial services to assist in. If you are injured or become ill, either physically or.
Workers’ Compensation Claim Form (DWC 1) & Notice of Potential
How my case is resolved. Specifically authorized by section 440.185(2), florida statutes. Number workers' compensation claim form. 6/10 if you are injured or become ill, either physically or. On the form, you will need to only fill out the “employee” section, which asks for basic information:
20162021 Form CA DIR DWC 1 Fill Online, Printable, Fillable, Blank
Web the division of workers' compensation (dwc) monitors the administration of workers' compensation claims, and provides administrative and judicial services to assist in. How i return to work. Give this form to the employee and have them. 6/10 if you are injured or become ill, either physically or. Number workers' compensation claim form.
You Can Obtain A Copy Of The California Dwc 1 Claim Form Here.
A dwc 1 is the form that is filled out to report an injury to your employer, and officially initiate a workers’ compensation claim. Web workers' compensation claim form (dwc 1) & notice of potential eligibility formulario de reclamo de compensación para trabajadores (dwc 1) y notificación de posible. 6/10 if you are injured or become ill, either physically or. Number workers' compensation claim form.
Web The Division Of Workers' Compensation (Dwc) Monitors The Administration Of Workers' Compensation Claims, And Provides Administrative And Judicial Services To Assist In.
File a claim form to protect your rights and start the workers’ compensation process. On the form, you will need to only fill out the “employee” section, which asks for basic information: If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be. Web find common forms used during the claims process and throughout your policy period.
Give This Form To The Employee And Have Them.
Web texas department of insurance Web formulario de reclamo de compensación de trabajadores (dwc 1) y notificación de posible elegibilidad rev. Web the employeris required to file an employer's first report of injury or illness. Specifically authorized by section 440.185(2), florida statutes.
How My Case Is Resolved.
1/1/2016 page 1 of 3. How i return to work. Web formulario de reclamo de compensación de trabajadores (dwc 1) y notificación de posible elegibilidad if you are injured or become ill, either physically or mentally,. Claims and return to work.