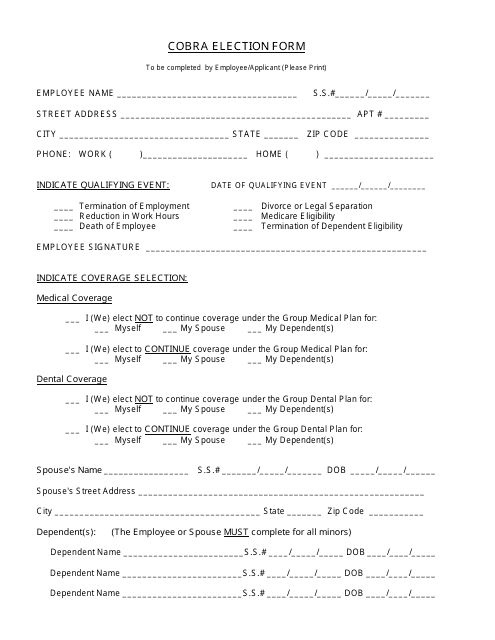
Cobra Continuation Coverage Election Form
Cobra Continuation Coverage Election Form - Cobra enrollee information name social security number address number and street. Web cobra continuation coverage factsheet. Web fill online, printable, fillable, blank cobra continuation coverage election form form. Nys department of civil service, employee benefits division attn: Web to elect cobra or retiree continuation coverage, complete this form and return it to the human resources department, county of york, 224 ballard street, p.o. Please complete this form if you wish to continue your current kaiser permanente benefits and. Please read the information in this notice very carefully before you make your decision. Therefore, you must complete the entire form, including the. Web cobra election form california department of human resources state of california 1. Web employers may use the model cobra continuation coverage notice in connection with extended election periods for qualified beneficiaries currently enrolled in.
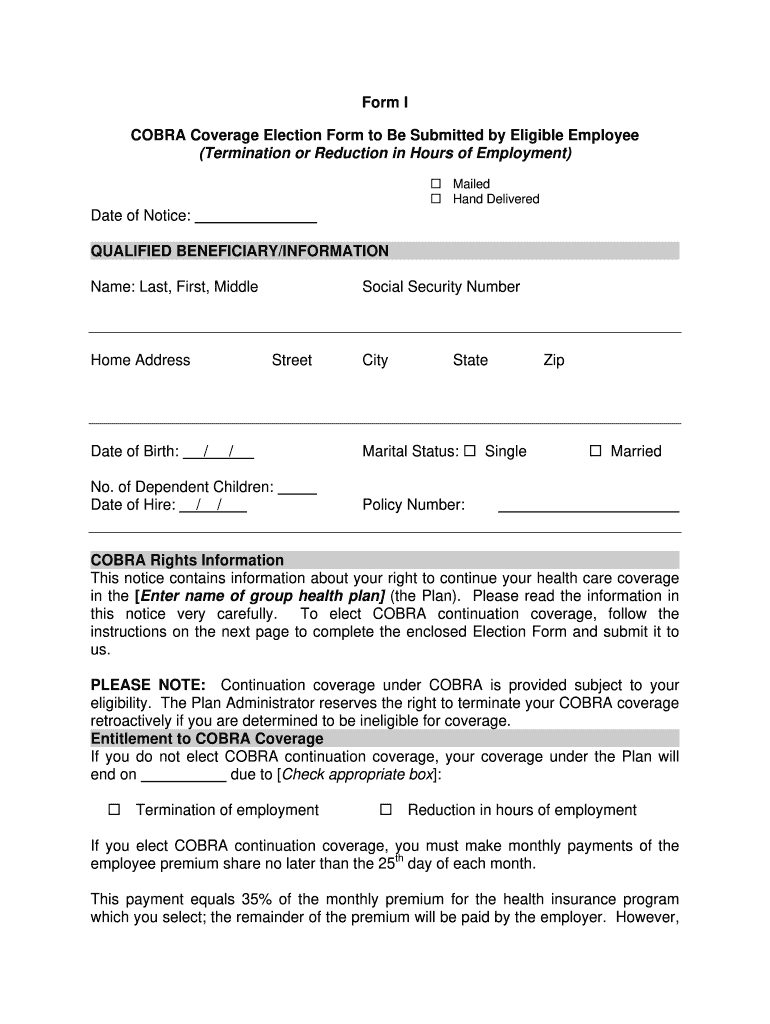
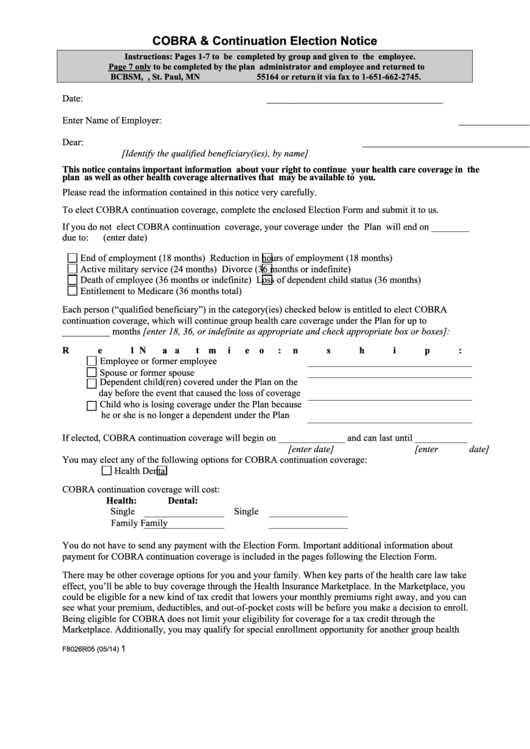
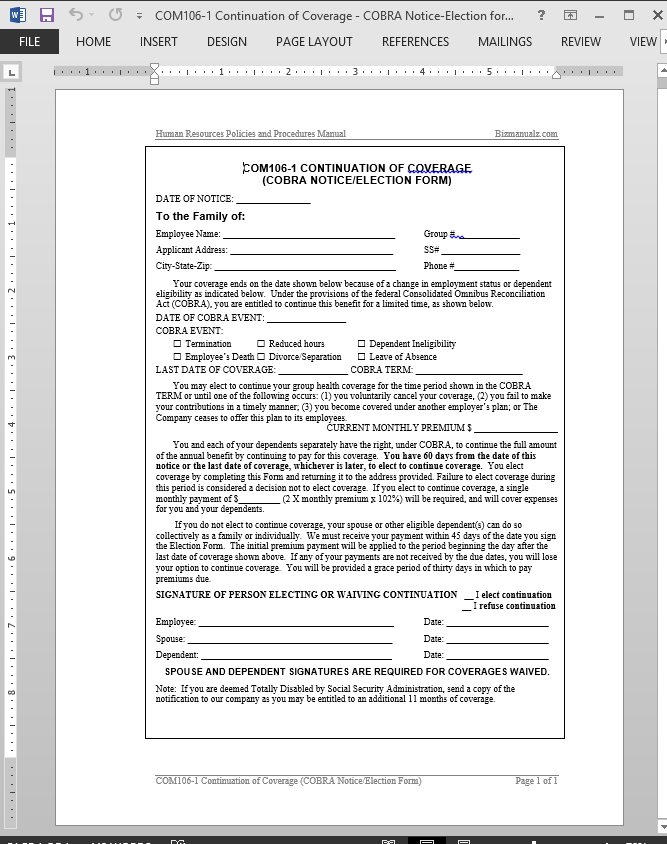
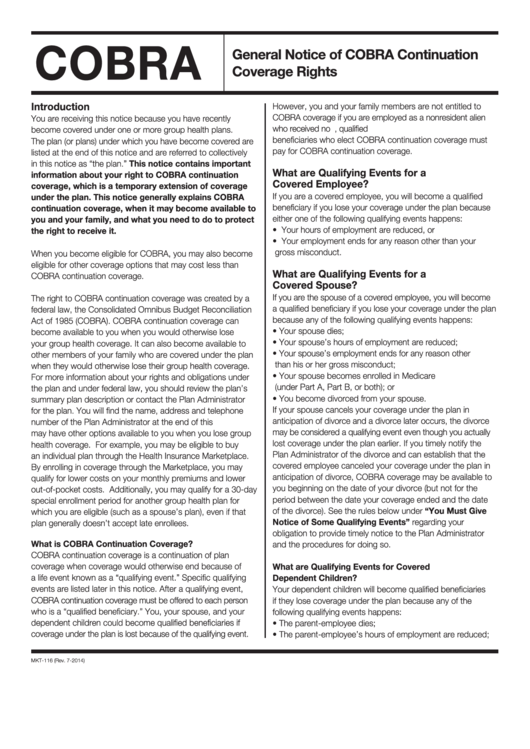
Web election to accept cobra. Nys department of civil service, employee benefits division attn: Covered employee and/or spouse and dependents checks election box to accept continuation of coverage. Web the consolidated omnibus budget reconciliation act (cobra) gives workers and their families who lose their health benefits the right to choose to continue group health. Web if you are currently enrolled in cobra continuation coverage. After receiving a notice of a qualifying event, the plan must provide the qualified beneficiaries with an election notice within 14. Web within 14 days of that notification, the plan administrator is required to notify the individual of his or her cobra rights. Use fill to complete blank online others pdf forms for free. If the employer also is the plan administrator and issues. Guidance for factsheet provides information about cobra continuation coverage, with a focus on the.
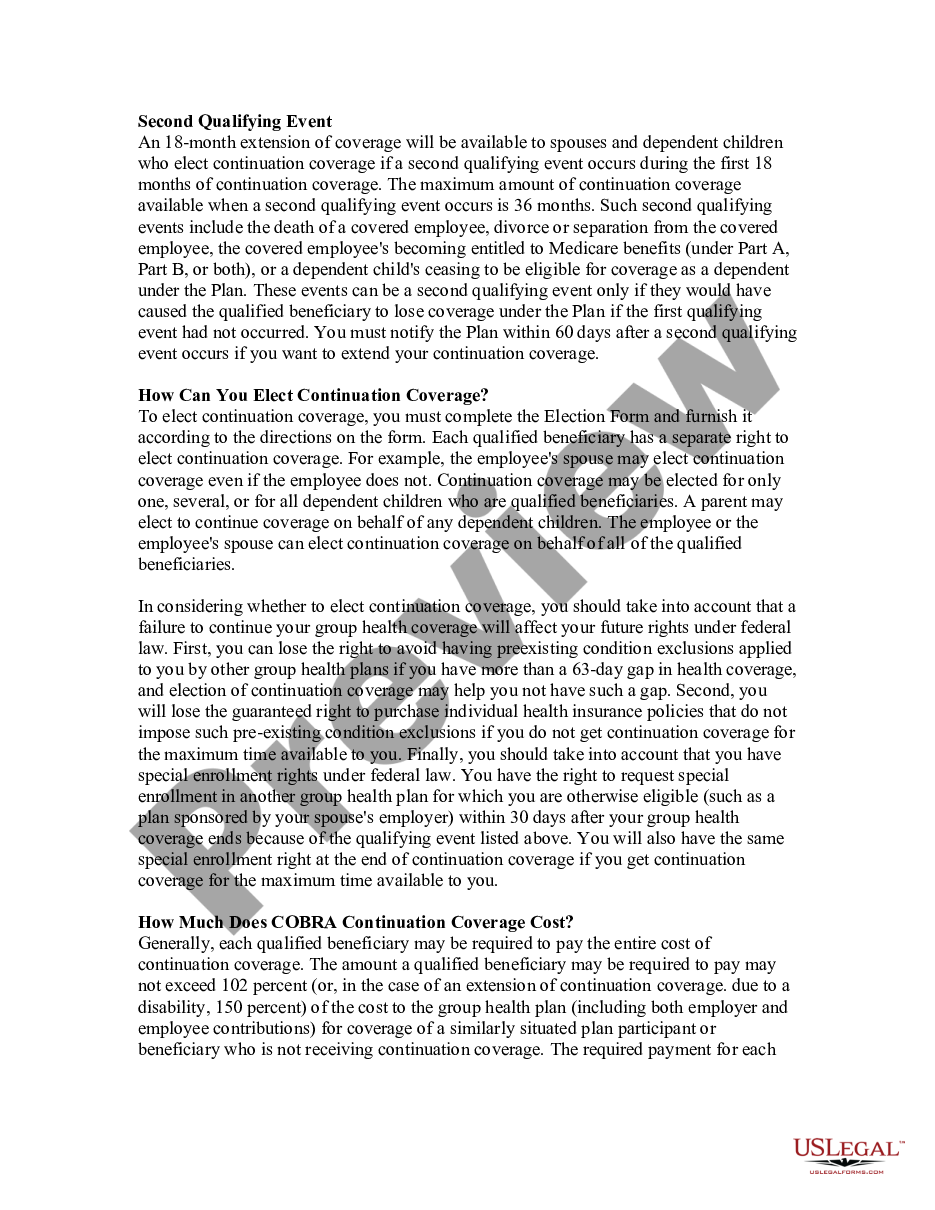
Web to elect cobra continuation coverage, complete this election form and return it to: Please complete this form if you wish to continue your current kaiser permanente benefits and. This also indicates acceptance of. Use fill to complete blank online others pdf forms for free. Web if you elect cobra continuation coverage, some options that were available to you before electing cobra coverage may still be available after cobra coverage is exhausted. Covered employee and/or spouse and dependents checks election box to accept continuation of coverage. Web cobra continuation coverage factsheet. Please read the information in this notice very carefully before you make your decision. Cobra enrollee information name social security number address number and street. Web employers may use the model cobra continuation coverage notice in connection with extended election periods for qualified beneficiaries currently enrolled in.
Cobra Election Form Download Printable PDF Templateroller
Election form your kaiser permanente benefits will terminate on. Web this form replaces all pebb continuation coverage (cobra) election/change forms previously submitted. Web election to accept cobra. Web instead of employees being required to elect cobra coverage within 60 days of losing group health coverage, plans are now required to “disregard” the period between march. Web if you are currently.
Fillable Cobra Notification Fill Out and Sign Printable PDF Template
Web this form replaces all pebb continuation coverage (cobra) election/change forms previously submitted. Therefore, you must complete the entire form, including the. Web to elect cobra or retiree continuation coverage, complete this form and return it to the human resources department, county of york, 224 ballard street, p.o. Web instead of employees being required to elect cobra coverage within 60.
Form F8026r05 Cobra & Continuation Election Notice printable pdf download
Web cobra requires continuation coverage to be offered to covered employees, their spouses, former spouses, and dependent children when group health coverage would. If the employer also is the plan administrator and issues. Web election to accept cobra. Web within 14 days of that notification, the plan administrator is required to notify the individual of his or her cobra rights..

Cobra Continuation Fill Online, Printable, Fillable, Blank pdfFiller
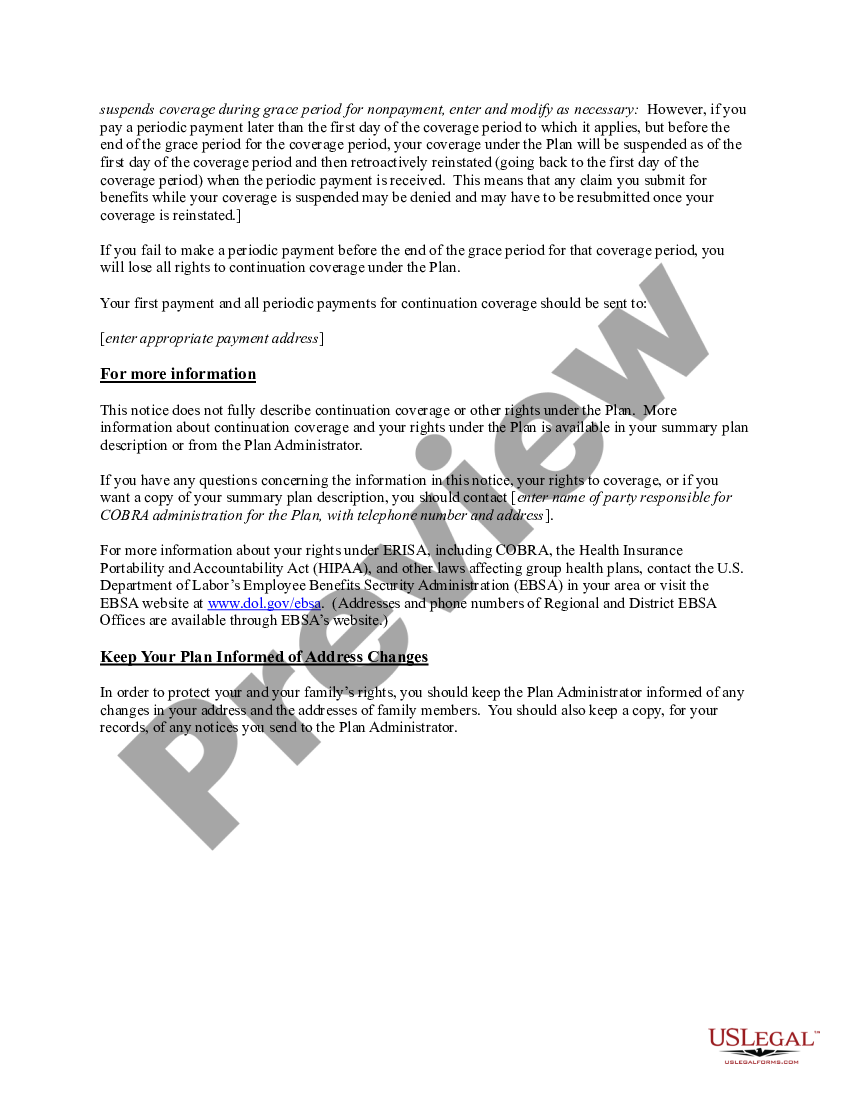
Therefore, you must complete the entire form, including the. Web fill online, printable, fillable, blank cobra continuation coverage election form form. Web cobra requires continuation coverage to be offered to covered employees, their spouses, former spouses, and dependent children when group health coverage would. After receiving a notice of a qualifying event, the plan must provide the qualified beneficiaries with.
Cobra Continuation of Coverage Request Template
Covered employee and/or spouse and dependents checks election box to accept continuation of coverage. Web to elect cobra continuation coverage, complete this election form and return it to: Therefore, you must complete the entire form, including the. Web within 14 days of that notification, the plan administrator is required to notify the individual of his or her cobra rights. Please.
Bcbs General Notice Of Cobra Continuation Coverage Rights Instruction
Election form your kaiser permanente benefits will terminate on. Please read the information in this notice very carefully before you make your decision. Use fill to complete blank online others pdf forms for free. This also indicates acceptance of. Web the consolidated omnibus budget reconciliation act (cobra) gives workers and their families who lose their health benefits the right to.
COBRA Continuation Coverage Election Notice Cobra Notice US Legal Forms
Please complete this form if you wish to continue your current kaiser permanente benefits and. Web employers may use the model cobra continuation coverage notice in connection with extended election periods for qualified beneficiaries currently enrolled in. Nys department of civil service, employee benefits division attn: Web cobra continuation coverage factsheet. Covered employee and/or spouse and dependents checks election box.
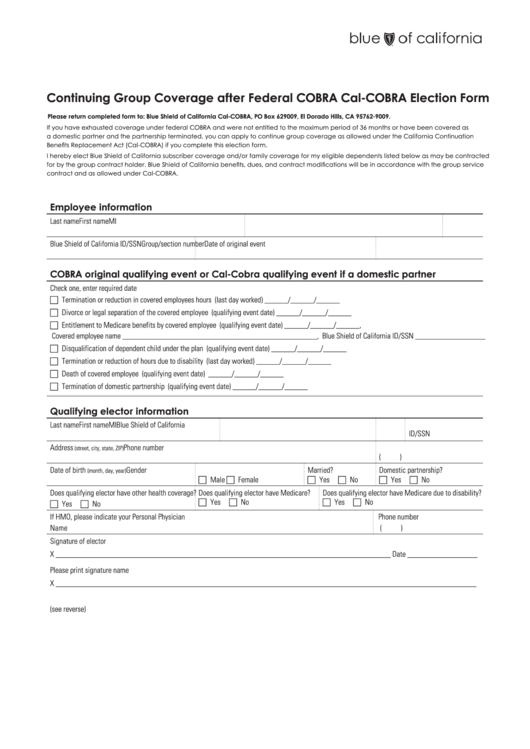
Continuing Group Coverage After Federal Cobra CalCobra Election Form
Use fill to complete blank online others pdf forms for free. Please complete this form if you wish to continue your current kaiser permanente benefits and. Covered employee and/or spouse and dependents checks election box to accept continuation of coverage. Web to elect cobra or retiree continuation coverage, complete this form and return it to the human resources department, county.
Model COBRA Continuation Coverage Election Notice Cobra Notice US
If the employer also is the plan administrator and issues. Therefore, you must complete the entire form, including the. Web this form replaces all pebb continuation coverage (cobra) election/change forms previously submitted. Please read the information in this notice very carefully before you make your decision. Web employers may use the model cobra continuation coverage notice in connection with extended.

COBRA election notices
Please read the information in this notice very carefully before you make your decision. Web the consolidated omnibus budget reconciliation act (cobra) gives workers and their families who lose their health benefits the right to choose to continue group health. If the employer also is the plan administrator and issues. This also indicates acceptance of. Web to elect cobra continuation.
Web This Form Replaces All Pebb Continuation Coverage (Cobra) Election/Change Forms Previously Submitted.
Web to elect cobra continuation coverage, complete this election form and return it to: Covered employee and/or spouse and dependents checks election box to accept continuation of coverage. Web the consolidated omnibus budget reconciliation act (cobra) gives workers and their families who lose their health benefits the right to choose to continue group health. Web cobra continuation coverage factsheet.
Use Fill To Complete Blank Online Others Pdf Forms For Free.
Please read the information in this notice very carefully before you make your decision. If the employer also is the plan administrator and issues. Web cobra election form california department of human resources state of california 1. After receiving a notice of a qualifying event, the plan must provide the qualified beneficiaries with an election notice within 14.
Web If You Elect Cobra Continuation Coverage, Some Options That Were Available To You Before Electing Cobra Coverage May Still Be Available After Cobra Coverage Is Exhausted.
Election form your kaiser permanente benefits will terminate on. Web within 14 days of that notification, the plan administrator is required to notify the individual of his or her cobra rights. This also indicates acceptance of. Guidance for factsheet provides information about cobra continuation coverage, with a focus on the.
If You Now Choose To Elect.
Cobra enrollee information name social security number address number and street. Web if you are currently enrolled in cobra continuation coverage. Please complete this form if you wish to continue your current kaiser permanente benefits and. Therefore, you must complete the entire form, including the.