Charity Care Application Form Nj
Charity Care Application Form Nj - Web purposes directly related to my eligibility for the new jersey hospital care program (charity care) and/or new jersey medicaid. Web to complete a financial assistance application, you will need the following documents: Web click on the links below to download/print our charity care forms and fact sheets. Charity care program department of health p.o. Web the way to fill out the meridian charity care application form on the web: Web who is eligible for charity care? Charity care fact sheet (english) charity care fact sheet (spanish) Web new jersey hospital care payment assistance program application for participation proof of identification, proof of income, and proof of assets must accompany this application. Web to find out if you qualify, you must fill out an application. Web locate charity care application and click get form to get started.
Use the tools we offer to submit your form. Web purposes directly related to my eligibility for the new jersey hospital care program (charity care) and/or new jersey medicaid. Photostat copies of the authorization will be. Sign online button or tick the preview image of the blank. Web home sfhcc home applying for charity care while all services provided in the student family healthcare center are provided free of charge often times patients require blood. You will be eligible for full. Web the new jersey hospital care payment assistance program (charity care assistance) is free or reduced charge care which is provided to patients who receive inpatient and. To be eligible for charity care, you must meet the following requirements: Proper patient and family identification documents. Web click on the links below to download/print our charity care forms and fact sheets.
You may apply for financial aid within 1 year after discharge from the hospital or receipt of outpatient care. Highlight relevant paragraphs of your documents or blackout delicate. Charity care program department of health p.o. To qualify you must meet both the income. This can include any of the following:. Proper patient and family identification documents. Web morristown nj 07960 summit, nj 07902 newton, nj 07860 pompton plains, nj 07444 hackettstown, nj 07840 it is your responsibility to submit all the documents requested. Charity care fact sheet (english) charity care fact sheet (spanish) Photostat copies of the authorization will be. Web enclosed please find your charity care/financial aid application forms.

New jersey hospital assistance program Fill out & sign online DocHub
Proper patient and family identification documents. Web who is eligible for charity care? Use the tools we offer to submit your form. Sign online button or tick the preview image of the blank. Web purposes directly related to my eligibility for the new jersey hospital care program (charity care) and/or new jersey medicaid.

Charity Care Nj Eligibility 2021 Is Charity Care Considered
Web the new jersey hospital care payment assistance program (charity care) is available to patients for inpatient and outpatient services at all acute care hospitals throughout new. To qualify you must meet. To be eligible for charity care, you must meet the following requirements: To qualify you must meet both the income. Call or visit your local hospital's business or.

Unc Charity Care Application 20202022 Fill and Sign Printable
Web the new jersey hospital care payment assistance program (charity care assistance) is free or reduced charge care which is provided to patients who receive inpatient and. This can include any of the following:. Charity care program department of health p.o. To qualify you must meet. Web to complete a financial assistance application, you will need the following documents:
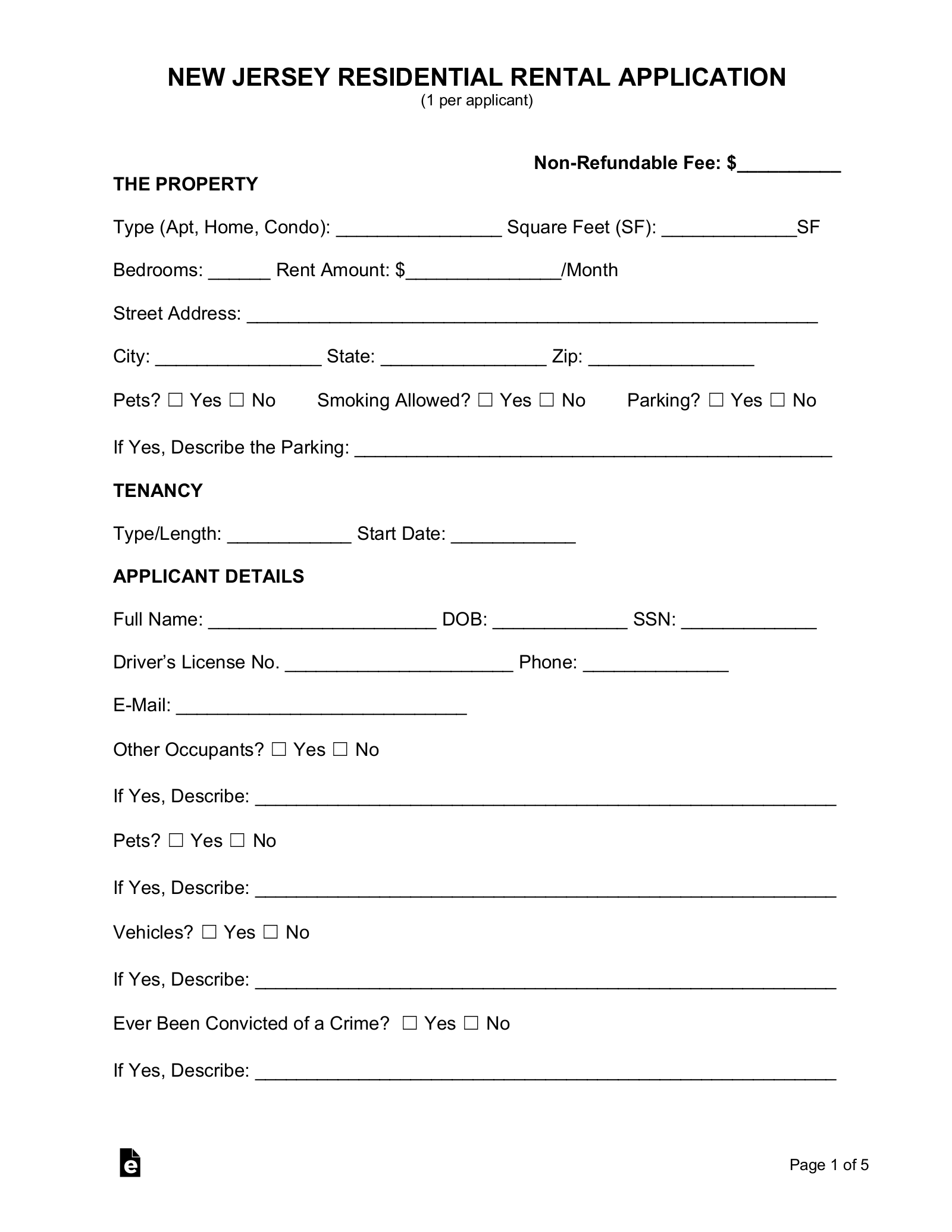
Free New Jersey Rental Application Form Word PDF eForms
Charity care program department of health p.o. Web the new jersey hospital care payment assistance program (charity care assistance) is free or reduced charge care which is provided to patients who receive inpatient and. Use the tools we offer to submit your form. Highlight relevant paragraphs of your documents or blackout delicate. Web who is eligible for charity care?

Online Donation Form Template JotForm
Web to find out if you qualify, you must fill out an application. Web home sfhcc home applying for charity care while all services provided in the student family healthcare center are provided free of charge often times patients require blood. Sign online button or tick the preview image of the blank. Photostat copies of the authorization will be. Use.

Kirklin Clinics Patient Charity Care Application Digital Library
To qualify you must meet both the income. Web who is eligible for charity care? To get started on the blank, utilize the fill camp; This can include any of the following:. Web new jersey hospital care payment assistance program application for participation proof of identification, proof of income, and proof of assets must accompany this application.
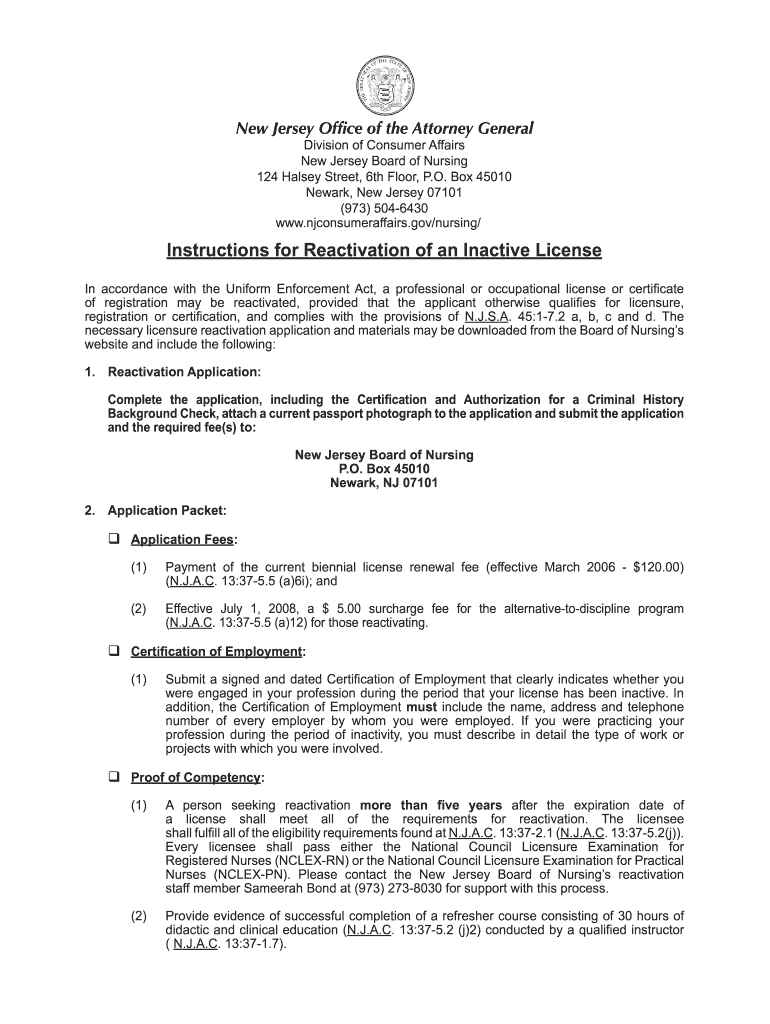
Nj Medical License Application PDF Form Fill Out and Sign Printable
Web to find out if you qualify, you must fill out an application. Web the new jersey hospital care payment assistance program (charity care assistance) is free or reduced charge care which is provided to patients who receive inpatient and. To qualify you must meet both the income. To be eligible for charity care, you must meet the following requirements:.
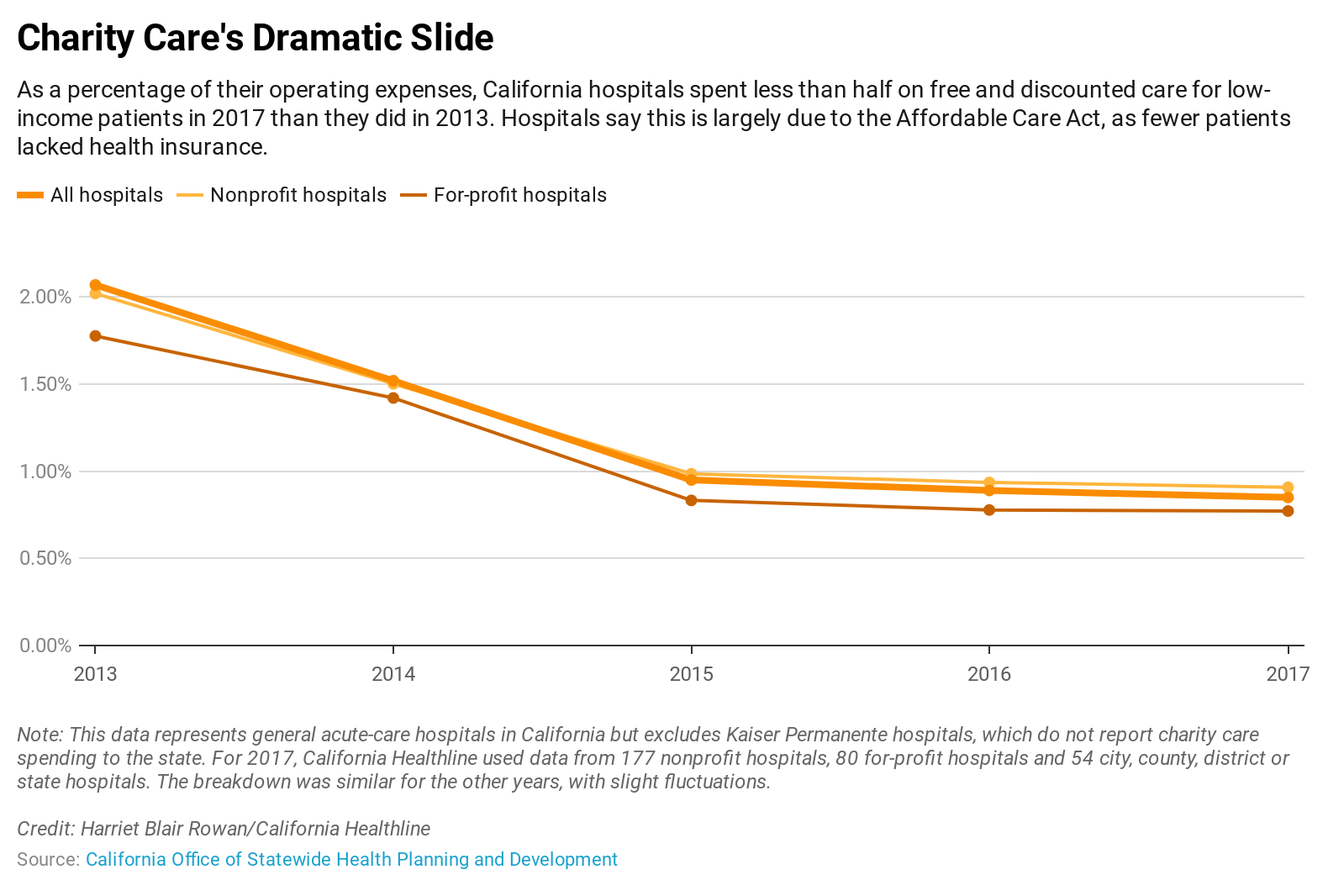
Charity Care Spending By Hospitals Plunges California Healthline
This can include any of the following:. Photostat copies of the authorization will be. Web click on the links below to download/print our charity care forms and fact sheets. Web to complete a financial assistance application, you will need the following documents: You will be eligible for full.
Medicaid Nj Application Forms Form Resume Examples E4Y4DBrYlB
Highlight relevant paragraphs of your documents or blackout delicate. Web purposes directly related to my eligibility for the new jersey hospital care program (charity care) and/or new jersey medicaid. Web click on the links below to download/print our charity care forms and fact sheets. Box 360 trenton nj 08625. Web morristown nj 07960 summit, nj 07902 newton, nj 07860 pompton.
Free New Jersey Rental Application Form PDF
Web charity care is available to new jersey residents who are uninsured, underinsured, or ineligible for state and federal programs. Web purposes directly related to my eligibility for the new jersey hospital care program (charity care) and/or new jersey medicaid. You may apply for financial aid within 1 year after discharge from the hospital or receipt of outpatient care. To.
Web New Jersey Hospital Care Assistant Program, Chairty Care, Cc Application Created Date:
Web home sfhcc home applying for charity care while all services provided in the student family healthcare center are provided free of charge often times patients require blood. Charity care fact sheet (english) charity care fact sheet (spanish) This can include any of the following:. Complete the application form, attach a copy of your latest paycheck stub or income source and.
Web The Way To Fill Out The Meridian Charity Care Application Form On The Web:
To qualify you must meet. Charity care program department of health p.o. Highlight relevant paragraphs of your documents or blackout delicate. You will be eligible for full.
Web To Find Out If You Qualify, You Must Fill Out An Application.
Web the new jersey hospital care payment assistance program (charity care assistance) is free or reduced charge care which is provided to patients who receive inpatient and. Use the tools we offer to submit your form. Web enclosed please find your charity care/financial aid application forms. Web morristown nj 07960 summit, nj 07902 newton, nj 07860 pompton plains, nj 07444 hackettstown, nj 07840 it is your responsibility to submit all the documents requested.
Proper Patient And Family Identification Documents.
Web new jersey hospital care payment assistance program application for participation proof of identification, proof of income, and proof of assets must accompany this application. Photostat copies of the authorization will be. Box 360 trenton nj 08625. To qualify you must meet both the income.