Ada Claim Form Fillable
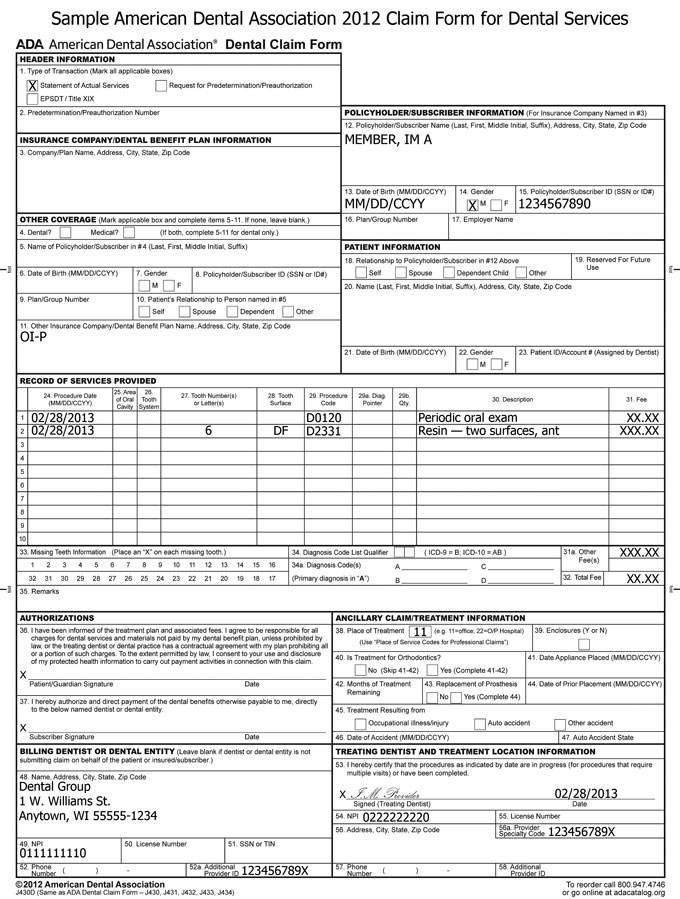
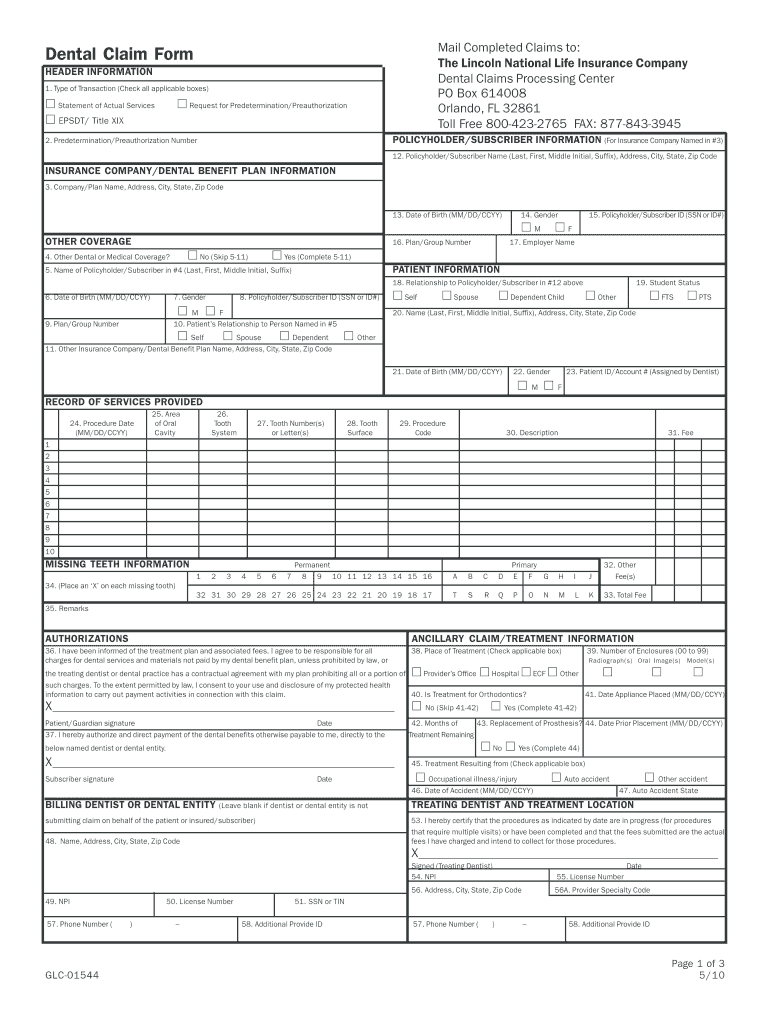
Ada Claim Form Fillable - Get your online template and fill it in using progressive features. Five relevant extracts from that. Get your online template and fill it in using progressive features. Ad download or email ada j430 & more fillable forms, register and subscribe now! Enjoy smart fillable fields and interactivity. U = unknown coordination of benefits (cob) when a claim is being. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into. Web print and fill out the ada dental claim form. Policyholder/subscriber name (last, first, middle initial, suffix), address, city, state, zip code 13. Date of birth (mm/dd/ccyy) 14.
Type text, add images, blackout confidential details, add comments, highlights and more. Web ada dental claim form instructions the following information highlights certain va specific form completion instructions. Comprehensive ada dental claim form completion instructions are printed in the cdt manual. Policyholder/subscriber name (last, first, middle initial, suffix), address, city, state, zip code 13. Web ★ 4.8 satisfied 59 votes how to fill out and sign 2012 dental claim form online? Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into. Ad free shipping on qualified orders. Five relevant extracts from that. The ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the. Edit your ada dental claim form printable online.
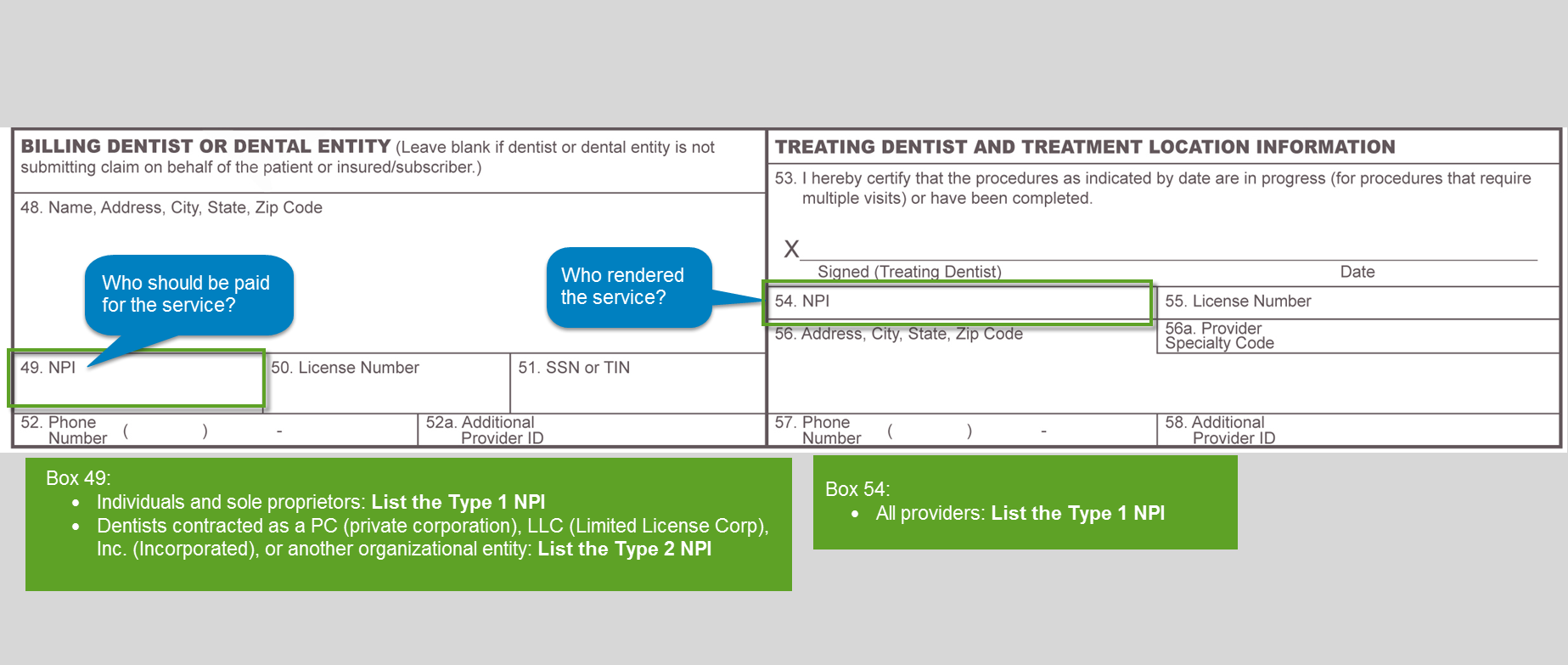
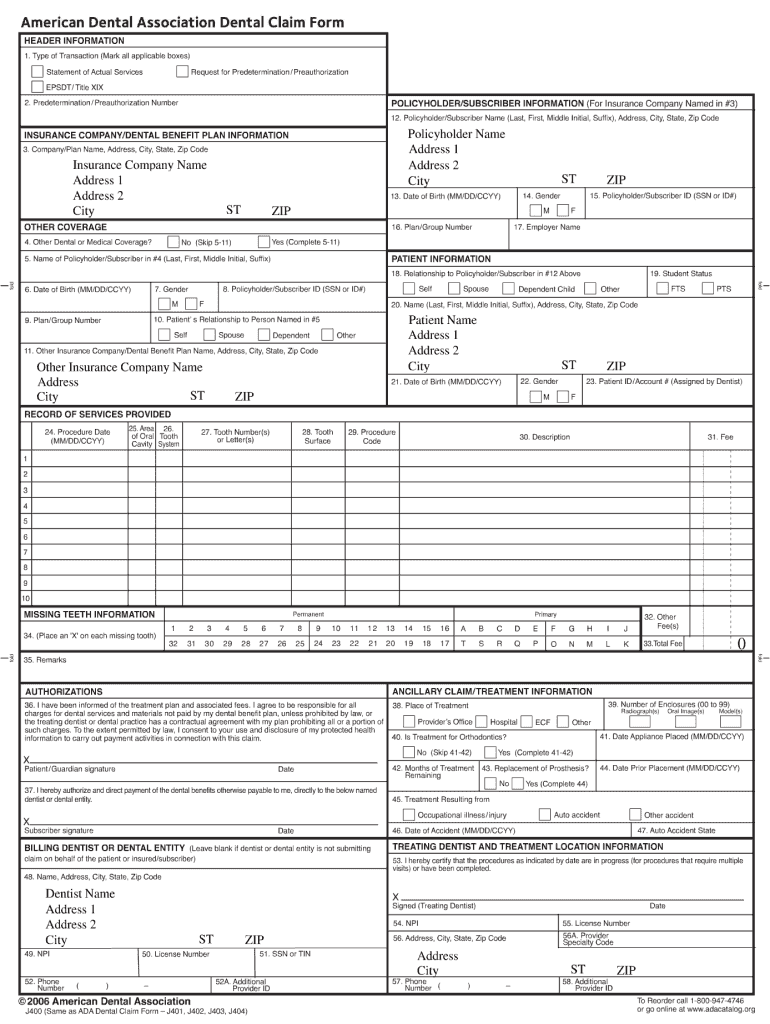
Web an employer is subject to the ada if it has 15 or more employees for 20 weeks of the current or preceding calendar year. Web complete ada claim form fillable and printable pdf online with us legal forms. Web print and fill out the ada dental claim form. Edit your ada dental claim form printable online. Web dental claim form header information type of transaction (mark all applicable boxes) statement of actual services request for. Web ada dental claim form sample unless the following sections of a dental bill are completed correctly, the bill will be returned and payment may be delayed. Sign it in a few clicks. Link opens in new window. Ad ada j400 form & more fillable forms, register and subscribe now! Find deals and low prices on ada claim forms at amazon.com

New ADA Dental Claim Form Requirements DentiMax
Sign it in a few clicks. Web the following information highlights certain form completion instructions. Date of birth (mm/dd/ccyy) 14. Any updates to these instructions will be posted on the ada’s web site. Web comprehensive ada dental claim form completion instructions are printed in the cdt manual.
Office Support
Web ada dental claim form instructions the following information highlights certain va specific form completion instructions. Any updates to these instructions will be posted on the ada’s web site. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into. Five relevant extracts.
Enjoy smart fillable fields and interactivity. Any updates to these instructions will be posted on the ada’s web site. Type text, add images, blackout confidential details, add comments, highlights and more. Ad ada j400 form & more fillable forms, register and subscribe now! Web a separate, fully completed claim form.
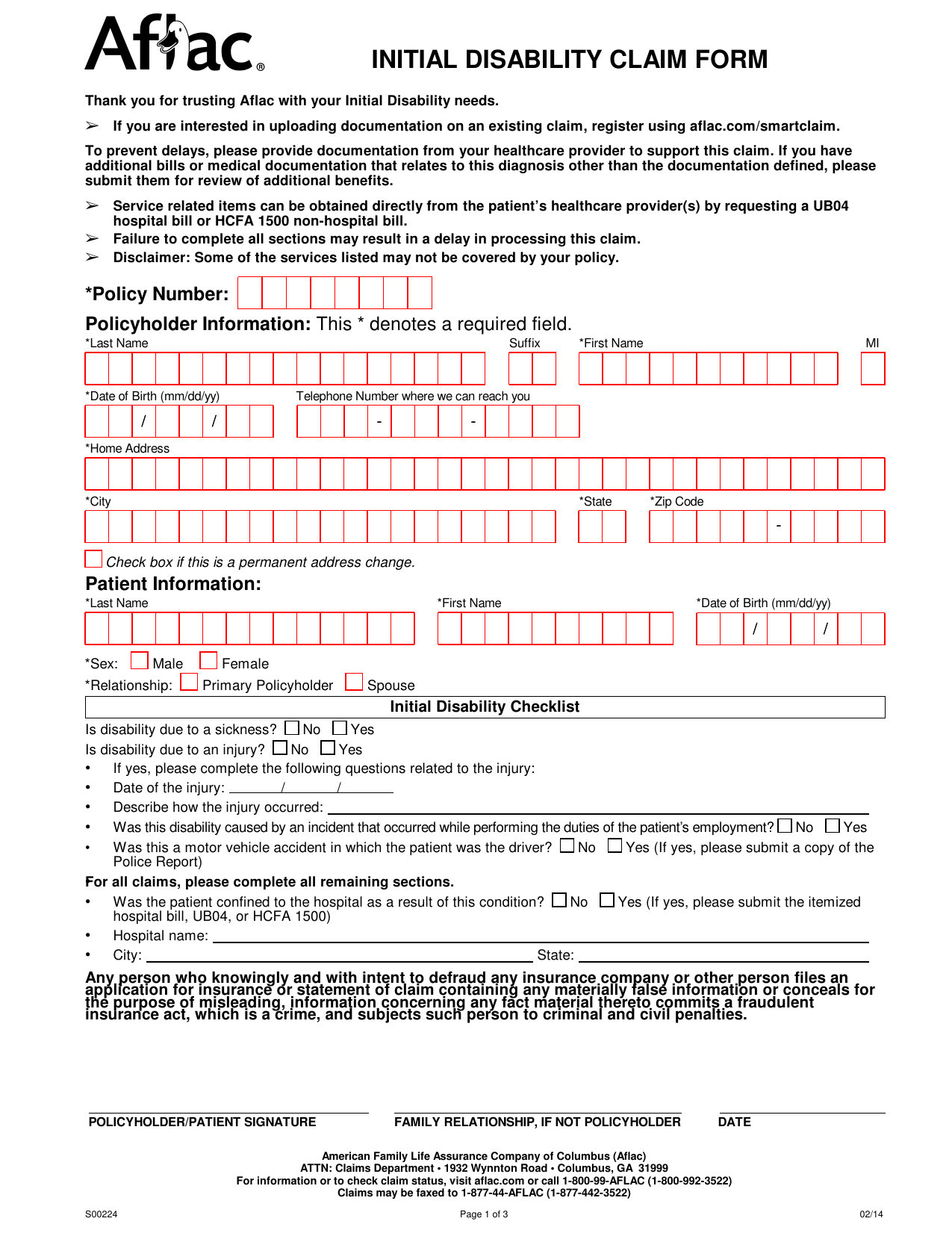
Download Aflac Short Term Disability Claim Form/ Initial Disability
Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. Web complete ada claim form fillable and printable pdf online with us legal forms. Ad download or email ada j430 & more fillable forms, register and subscribe now! Web how to fill out and sign blank ada claim form 2022 online? Edit your ada dental claim.
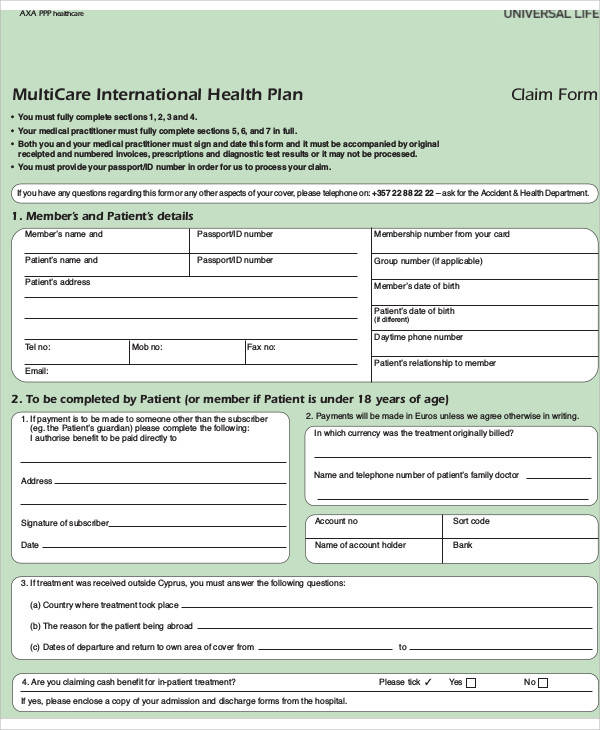
FREE 47+ Claim Forms in PDF
Web ada dental claim form instructions the following information highlights certain va specific form completion instructions. Comprehensive ada dental claim form. U = unknown coordination of benefits (cob) when a claim is being. Web ada dental claim form sample unless the following sections of a dental bill are completed correctly, the bill will be returned and payment may be delayed..

Physicians Mutual Insurance Company Dental Insurance Claim Form. Dental
Link opens in new window. Web how to fill out and sign blank ada claim form 2022 online? Save or instantly send your ready documents. Web ada dental claim form sample unless the following sections of a dental bill are completed correctly, the bill will be returned and payment may be delayed. Comprehensive ada dental claim form.
Printable Ada Dental Claim Form 2021 Fill Out and Sign Printable PDF
Web a separate, fully completed claim form. Link opens in new window. Five relevant extracts from that. Ad free shipping on qualified orders. Find deals and low prices on ada claim forms at amazon.com
Free Printable Ada Dental Claim Form templates.iesanfelipe.edu.pe
Enjoy smart fillable fields and interactivity. Link opens in new window. Print and fill out the appointment of representative. Web an employer is subject to the ada if it has 15 or more employees for 20 weeks of the current or preceding calendar year. Free, easy returns on millions of items.
Dental Claim Form Fill Out and Sign Printable PDF Template signNow
Sign it in a few clicks. Type text, add images, blackout confidential details, add comments, highlights and more. Date of birth (mm/dd/ccyy) 14. Edit your ada dental claim form printable online. Employers under the ada must reasonably accommodate.
Ada Dental Claim Form Fillable Fill Out and Sign Printable PDF
Web comprehensive ada dental claim form completion instructions are printed in the cdt manual. Employers under the ada must reasonably accommodate. U = unknown coordination of benefits (cob) when a claim is being. Policyholder/subscriber name (last, first, middle initial, suffix), address, city, state, zip code 13. Web ada dental claim form instructions the following information highlights certain va specific form.
Ad Free Shipping On Qualified Orders.
Web ada dental claim form sample unless the following sections of a dental bill are completed correctly, the bill will be returned and payment may be delayed. Web an employer is subject to the ada if it has 15 or more employees for 20 weeks of the current or preceding calendar year. Date of birth (mm/dd/ccyy) 14. The ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the.
Edit Your Ada Dental Claim Form Printable Online.
Sign it in a few clicks. Print and fill out the appointment of representative. Web complete ada claim form fillable and printable pdf online with us legal forms. Link opens in new window.
Web Object Moved This Document May Be Found Here
Web the following information highlights certain form completion instructions. Ad download or email ada j430 & more fillable forms, register and subscribe now! Web ada dental claim form instructions the following information highlights certain va specific form completion instructions. Policyholder/subscriber name (last, first, middle initial, suffix), address, city, state, zip code 13.
Employers Under The Ada Must Reasonably Accommodate.
Link opens in new window. Any updates to these instructions will be posted on the ada’s web site. Easily fill out pdf blank, edit, and sign them. Web dental claim form header information type of transaction (mark all applicable boxes) statement of actual services request for.